علوم اعصاب شناختی؛ کنترل شناختی: کارکرد اجرایی

دعای مطالعه [ نمایش ]
بِسْمِ الله الرَّحْمنِ الرَّحیمِ
اَللّهُمَّ اَخْرِجْنى مِنْ ظُلُماتِ الْوَهْمِ
خدايا مرا بيرون آور از تاريكىهاى وهم،
وَ اَكْرِمْنى بِنُورِ الْفَهْمِ
و به نور فهم گرامى ام بدار،
اَللّهُمَّ افْتَحْ عَلَيْنا اَبْوابَ رَحْمَتِكَ
خدايا درهاى رحمتت را به روى ما بگشا،
وَانْشُرْ عَلَيْنا خَزائِنَ عُلُومِكَ بِرَحْمَتِكَ يا اَرْحَمَ الرّاحِمينَ
و خزانههاى علومت را بر ما باز كن به امید رحمتت اى مهربانترين مهربانان.

If everything seems under control, you’re just not going fast enough. Maria Andreti
اگر به نظر میرسد همه چیز تحت کنترل است، شما به اندازه کافی سریع پیش نمیروید. ماریا آندرتی
BIG Questions
▪️ What are the computational requirements that enable organisms to plan and execute complex behaviors?
▪️ What are the neural mechanisms that support working memory, and how
is task-relevant information selected?
▪️How does the brain represent the value associated with different sensory events and experiences, and how does it use this information to make decisions when faced with multiple options for taking action?
▪️ How do we monitor ongoing performance to help ensure the success of complex behaviors?
پرسشهای مهم
▪️ الزامات محاسباتی که موجودات زنده را قادر میسازد تا رفتارهای پیچیده را برنامه ریزی و اجرا کنند چیست؟
▪️ مکانیسمهای عصبی که از حافظه فعال پشتیبانی میکنند چیست و چگونه است آیا اطلاعات مربوط به کار انتخاب شده است؟
▪️ مغز چگونه ارزش مرتبط با رویدادها و تجربیات حسی مختلف را نشان میدهد و چگونه از این اطلاعات برای تصمیم گیری در هنگام مواجهه با گزینههای متعدد برای اقدام استفاده میکند؟
▪️ چگونه بر عملکرد جاری نظارت میکنیم تا از موفقیت رفتارهای پیچیده اطمینان حاصل کنیم؟
A SEASONED NEUROLOGIST was caught by surprise when his new patient, W.R., reported his main symptom quite simply: “I have lost my ego.” (R. T. Knight & Grabowecky, 1995).
یک نورولوژیست کارآزموده زمانی غافلگیر شد که بیمار جدیدش (دبلیو. آر.) علامت اصلی [بیماری] خود را خیلی ساده بیان کرد: «خودم را گم کردهام.» (آر.تی. نایت و گرابوفسکی).
A driven child, W.R. decided at an early age that he wanted to become a lawyer. Focused on this plan, he completed college with an excellent GPA and took the right classes for a prelaw student. He was accepted to his first-choice law school and graduated with a solid, if not stellar, academic record. But then his life derailed: Suddenly, he seemed to have forgotten his plan to work at a top law firm. Four years later, he had yet to look for a job in the legal profession and, in fact, had not taken the bar exam. Instead, he was an instructor at a tennis club.
دبلیو آر، کودکی مصمم بود و از سنین خردسالی تصمیم گرفت که وکیل شود. او با تمرکز بر این طرح، کالج را با معدل عالی به پایان رساند و کلاسهای پیش نیاز و مناسب برای دانشجویان حقوق را گذراند. او در اولین دانشکده حقوق انتخابی خود پذیرفته شد و با یک سوابق تحصیلی خوب، اگر نگوییم درخشان، فارغ التحصیل شد. اما پس از آن ناگهان مسیر زندگیش تغییر کرد و به نظر میرسید که برنامه خود را برای کار در برترین شرکت حقوقی فراموش کرده است. چهار سال بعد، او هنوز به دنبال شغلی در حرفه وکالت نبود و در واقع در آزمون وکالت شرکت نکرده بود. در عوض، او مربی یک باشگاه تنیس بود.
Accompanying W.R. at the neurologist’s office was his brother, who reported that the family had found W.R.’s behavior odd but not atypical of the times, perhaps indicative of an early, antimaterialist midlife crisis. Maybe he would find satisfaction in teaching tennis, his favorite hobby, or perhaps this was just a temporary diversion before he embarked on a career in law after all. But no: W.R. eventually gave up on his job and even lost interest in playing tennis. His nonchalant attitude frustrated his opponents, as he forgot to keep track of the score and whose turn it was to serve. Unable to support himself financially, W.R. hit up his brother with increasingly frequent requests for “temporary” loans.
برادر دبلیو. آر. که همراه او در مطب متخصص مغز و اعصاب بود، شرح داد که آن زمان خانواده تصور میکردند شاید رفتار عجیب و غریب اما غیرمعمول دبلیو. آر. نشان دهنده بحران میانسالی ضد مادی زودرس باشد. شاید تدریس سرگرمیمورد علاقهاش تنیس مایه خشنودی اوست، یا شاید این فقط یک سرگرمیموقت قبل از شروع حرفه حقوق باشد. اما این گونه نبود. دبلیو. آر. در نهایت کار خود را رها کرد و حتی علاقه خود را به بازی تنیس از دست داد. سهل انگاری او، طرف مقابلش را کلافه میکرد، زیرا او فراموش میکرد حساب امتیاز را نگه دارد و نوبت سرویس او است. دبلیو. آر. قادر به تأمین مالی خود نبود بنابراین درخواستهای مکرر فزایندهای از برادرش برای دریافت وام موقت داشت.
Clearly a highly intelligent man, W.R. was cognizant that something was amiss. Though he expressed repeatedly that he wished he could pull things together, he simply could not take the necessary steps to find a job or get a place to live. He had little regard for his own future, for his successes, even for his own happiness. His brother noted another radi- cal change in W.R.: He had not been on a date for a number of years and seemed to have lost all interest in romantic pursuits. W.R. sheepishly agreed.
واضح است که دبلیو آر که مردی بسیار باهوش بود، میدانست که چیزی اشتباه است. اگرچه او بارها ابراز داشت که آرزو دارد بتواند همه چیز را جمع و جور کند، اما به سادگی نمیتواند اقدامات لازم را برای یافتن شغل یا یافتن مکانی برای زندگی انجام دهد. او به آینده خود، به موفقیتهایش، حتی برای خوشبختی خود اهمیت چندانی نمیداد. برادرش به تغییر اساسی دیگری در دبلیو. آر. اشاره کرد: او چند سالی بود که قرار ملاقاتی نداشت و به نظر میرسید که علاقه خود را به کارهای عاشقانه از دست داده بود. دبلیو آر با شرمندگی موافقت کرد.
If this had been the whole story, the neurologist might have thought that a psychiatrist was a better option to treat a “lost ego.” However, during his last year in law school, W.R. had suffered a seizure. An extensive neurological examination at the time failed to identify the cause of the seizure, so it was diag- nosed as an isolated event, perhaps related to the fact that on the night before the seizure, W.R. had been drinking coffee all night while preparing for an exam.After hearing about the events of the previous 4 years, the neurologist decided it was time to reconsider the cause of the seizure.
اگر تمام داستان این بود، متخصص مغز و اعصاب ممکن بود فکر میکرد که روانپزشک گزینه بهتری برای درمان «خود گمشده» است. با این حال، در آخرین سال تحصیلی خود در دانشکده حقوق، دبلیو. آر. دچار تشنج شده بود. یک معاینه عصبی گسترده در آن زمان نتوانست علت تشنج را شناسایی کند، بنابراین به عنوان یک رویداد منفرد تشخیص داده شد، شاید به این واقعیت مربوط میشود که در شب قبل از تشنج، دبلیو. آر. تمام شب در حالی که آماده میشد قهوه مینوشید. پس از شنیدن رویدادهای 4 سال گذشته، متخصص مغز و اعصاب تصمیم گرفت که در مورد علت تشنج تجدید نظر کند.
ACT scan confirmed the neurologist’s worst fears. W.R.’s brain had an extremely large astrocytoma that had traversed along the fibers of the corpus callosum, extensively invading the lateral prefrontal cortex in the left hemisphere and a considerable portion of the right frontal lobe. This tumor had very likely caused the initial seizure and over the previous 4 years had slowly grown. The prognosis was now poor, with a life expectancy of about a year.
سی تی اسکن بدترین ترسهای متخصص مغز و اعصاب را تایید کرد. مغز دبلیو. آر. دارای یک آستروسیتوم بسیار بزرگ بود که در امتداد رشتههای جسم پینه ای عبور کرده بود و به طور گسترده به قشر پرهفرونتال جانبی در نیمکره چپ و بخش قابل توجهی از لوب پیشانی راست حمله میکرد. این تومور به احتمال زیاد باعث تشنج اولیه شده بود و در 4 سال گذشته به آرامیرشد کرده بود. پیش آگهی اکنون بد بود و امید به زندگی حدود یک سال بود.
W.R.’s brother was devastated on hearing the news. W.R., on the other hand, remained relatively passive and detached. Though he understood that the tumor was the culprit behind the dramatic life changes he had experienced, he was not angry or upset. Instead, he appeared unconcerned. He under- stood the seriousness of his condition, but the news, as with so many of his recent life events, failed to evoke a clear response or any resolve to take some action. W.R.’s self-diagnosis seemed to be right on target: He had lost his ego and, with it, the ability to take command of his own life.
برادر دبلیو آر با شنیدن این خبر بسیار ناراحت شد. از طرف دیگر، دبلیو. آر. نسبتاً منفعل و جدا باقی ماند. اگرچه او درک میکرد که تومور مقصر تغییرات چشمگیر زندگی است که تجربه کرده بود، عصبانی یا ناراحت نبود. در عوض، او بی توجه به نظر میرسید. او وخیم بودن وضعیت خود را درک میکرد، اما اخبار، مانند بسیاری از رویدادهای اخیر زندگیاش، نتوانست پاسخ روشنی یا تصمیمیبرای انجام برخی اقدامات را برانگیزد. به نظر میرسید که خود تشخیصی دبلیو آر دقیقاً هدف قرار گرفته بود: او نفس خود را از دست داده بود و به همراه آن توانایی کنترل زندگی خود را از دست داده بود.
In this chapter our focus turns to cognitive control processes, which are essential for the kind of behav- ior that is uniquely human, be it going to law school, playing tennis, or recognizing that something is amiss in one’s actions or those of a loved one. Cognitive con- trol processes give us the ability to override automatic thoughts and behavior and step out of the realm of habitual responses. They also give us cognitive flexibil- ity, letting us think and act in novel and creative ways.
در این فصل تمرکز ما به فرآیندهای کنترل شناختی معطوف میشود، که برای نوع رفتاری که منحصراً انسانی است، ضروری است، خواه رفتن به دانشکده حقوق، بازی تنیس، یا تشخیص اینکه چیزی در کارهای خود یا یکی از عزیزان اشتباه است. یکی فرآیندهای کنترل شناختی به ما این توانایی را میدهد که افکار و رفتار خودکار را نادیده بگیریم و از قلمرو پاسخهای معمولی خارج شویم. آنها همچنین به ما انعطافپذیری شناختی میدهند و به ما اجازه میدهند به شیوههای بدیع و خلاقانه فکر و عمل کنیم.
To facilitate discussion of these functions, we first review the anatomy of the frontal lobe and the behav- ioral problems that are observed when this region of the brain is damaged. We then focus on goal-oriented behavior and decision making, two complicated pro- cesses that rely on cognitive control mechanisms to work properly. And deciding on a goal is only the first step toward attaining it. Planning how to attain it and then sticking with the plan are also complicated affairs involving different cognitive control processes, which we examine in the final sections of this chapter.
برای تسهیل بحث در مورد این عملکردها، ابتدا آناتومی لوب فرونتال و مشکلات رفتاری را که در هنگام آسیب دیدن این ناحیه از مغز مشاهده میشود، مرور میکنیم. سپس بر رفتار هدفمدار و تصمیمگیری تمرکز میکنیم، دو فرآیند پیچیده که برای کارکرد صحیح به مکانیسمهای کنترل شناختی متکی هستند. و تصمیم گیری در مورد یک هدف تنها اولین قدم برای رسیدن به آن است. برنامه ریزی چگونگی دستیابی به آن و سپس پایبندی به برنامه نیز امور پیچیده ای است که شامل فرآیندهای کنترل شناختی مختلف است که در بخشهای پایانی این فصل به بررسی آنها میپردازیم.
12.1 The Anatomy Behind Cognitive Control
12.1 آناتومی پشت کنترل شناختی
Cognitive control, sometimes referred to as executive function, refers to the set of psychological processes that enable us to use our perceptions, knowledge, and goals to bias the selection of action and thoughts from a multitude of possibilities. Collectively, the behaviors thus enabled can be described as goal-oriented behavior, frequently requiring the coordination of a complex set of actions that may unfold over an extended period of time. The successful completion of goal-oriented behavior faces many chal- lenges, and cognitive control is necessary to meet them.
کنترل شناختی که گاهی به عنوان کارکرد اجرایی از آن یاد میشود، به مجموعه فرآیندهای روانشناختی اشاره دارد که ما را قادر میسازد تا از ادراکات، دانش و اهداف خود برای سوگیری انتخاب کنش و افکار از میان بسیاری از احتمالات استفاده کنیم. در مجموع، رفتارهایی که از این طریق فعال میشوند را میتوان به عنوان رفتار هدف گرا توصیف کرد که اغلب به هماهنگی مجموعه پیچیده ای از اقدامات نیاز دارد که ممکن است در یک دوره زمانی طولانی آشکار شود. تکمیل موفقیتآمیز رفتار هدفمحور با چالشهای زیادی مواجه است و کنترل شناختی برای رویارویی با آنها ضروری است.
All of us must develop a plan of action that draws on our personal experiences, yet is tailored to the current environment. Such actions must be flexible and adaptive to accommodate unforeseen changes and events. We must monitor our actions to stay on target and attain our goal, and we may need to inhibit a habitual response in order to do so. Although you might want to stop at the dough- nut shop when heading to work in the morning, cognitive control mechanisms can override that sugary urge.
همه ما باید یک برنامه عملی ایجاد کنیم که بر اساس تجربیات شخصی ما باشد، اما متناسب با محیط فعلی باشد. چنین اقداماتی باید انعطاف پذیر و سازگار باشند تا با تغییرات و رویدادهای پیش بینی نشده سازگاری داشته باشند. ما باید اقدامات خود را برای ماندن در هدف و رسیدن به هدف خود تحت نظر داشته باشیم، و ممکن است برای انجام این کار لازم باشد از یک واکنش معمولی جلوگیری کنیم. اگر چه ممکن است بخواهید هنگام رفتن به محل کار صبح در مغازه دونات فروشی توقف کنید، مکانیسمهای کنترل شناختی میتوانند بر این میل شیرین غلبه کنند.
As might be suspected of any complex process, cognitive control requires the integrated function of many different parts of the brain. This chapter highlights the frontal lobes. As we learned in Chapter 8, the most posterior part of the frontal lobe is the primary motor cortex (see the “Anatomical Orientation” box on p. 517). Anterior and ventral to the motor cortex are the secondary motor areas, made up of the lateral premotor cortex and the supplementary motor area. The remainder of the frontal lobe is termed the prefrontal cortex (PFC). We will refer to four regions of prefrontal cortex in this chapter: the lateral prefrontal cortex (LPFC), the frontal pole (FP), the orbitofrontal cortex (OFC) (sometimes referred to as the ventromedial zone), and the medial frontal cortex (MFC).
همانطور که ممکن است در مورد هر فرآیند پیچیده ای مشکوک شود، کنترل شناختی به عملکرد یکپارچه بسیاری از بخشهای مختلف مغز نیاز دارد. این فصل لوبهای فرونتال را برجسته میکند. همانطور که در فصل 8 آموختیم، خلفی ترین قسمت لوب فرونتال قشر حرکتی اولیه است (به کادر «جهت تشریح» در صفحه 517 مراجعه کنید). قدامیو شکمیقشر حرکتی نواحی حرکتی ثانویه هستند که از قشر پیش حرکتی جانبی و ناحیه حرکتی تکمیلی تشکیل شدهاند. باقیمانده لوب پیشانی قشر پیشانی (PFC) نامیده میشود. ما در این فصل به چهار ناحیه قشر پرهفرونتال اشاره خواهیم کرد: قشر پرهفرونتال جانبی (LPFC)، قطب پیشانی (FP)، قشر اوربیتوفرونتال (OFC) (گاهی اوقات به عنوان ناحیه شکمیمیانی شناخته میشود) و قشر پیشانی میانی (MFC).
In this chapter we concentrate on two prefrontal control systems. The first system, which includes the LPFC, OFC, and FP, supports goal-oriented behavior. This control system works in concert with more posterior regions of the cortex to constitute a working memory sys- tem that recruits and selects task-relevant information. This system is involved with planning; simulating consequences; and initiating, inhibiting, and shifting behavior.
در این فصل ما بر روی دو سیستم کنترل پرهفرونتال تمرکز میکنیم. اولین سیستم که شامل LPFC، OFC و FP میشود، از رفتار هدف گرا پشتیبانی میکند. این سیستم کنترل در هماهنگی با نواحی خلفی بیشتر قشر مغز کار میکند تا یک سیستم حافظه کاری را تشکیل دهد که اطلاعات مربوط به کار را جذب و انتخاب میکند. این سیستم با برنامه ریزی درگیر است. شبیه سازی پیامدها؛ و شروع، بازدارنده و تغییر رفتار.
ANATOMICA ORIENTATION
جهت تشریح
Anatomy of Cognitive Control
آناتومی کنترل شناختی
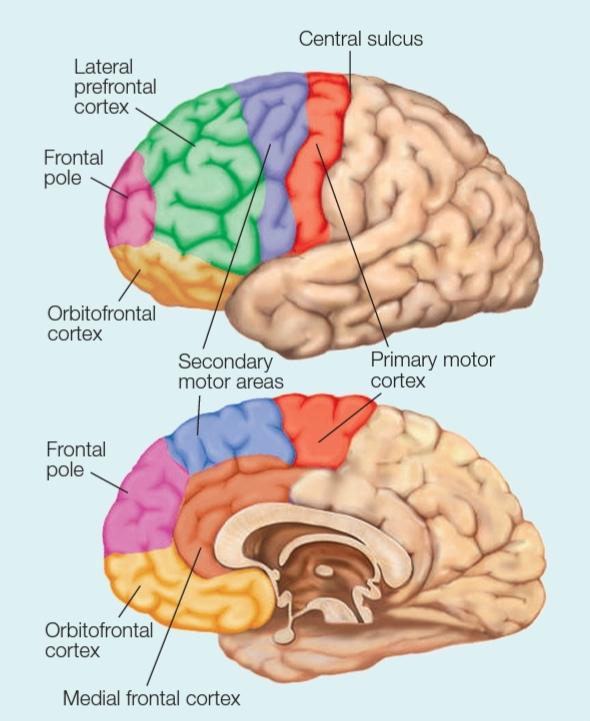
The prefrontal cortex includes all of the areas in front of the primary motor cortex and secondary motor areas. The four subdivisions of prefrontal cortex are the lateral prefrontal cortex, the frontal pole, the orbitofrontal cortex (which lies above the bony orbits of the eyes), and the medial frontal cortex.
قشر پرهفرونتال شامل تمام نواحی جلوی قشر حرکتی اولیه و نواحی حرکتی ثانویه است. چهار بخش فرعی قشر پرهفرونتال عبارتند از: قشر پرهفرونتال جانبی، قطب پیشانی، قشر اوربیتوفرونتال (که بالای مدارهای استخوانی چشمها قرار دارد) و قشر پیشانی میانی.
The second control system, which includes the MFC, plays an essential role in guiding and monitoring behavior. It works in tandem with the rest of the prefrontal cortex, monitoring ongoing activity to modulate the degree of cognitive control needed to keep behavior in line with current goals.
سیستم کنترل دوم که شامل MFC است، نقش اساسی در هدایت و نظارت بر رفتار ایفا میکند. این در کنار بقیه قشر پرهفرونتال عمل میکند و فعالیتهای مداوم را برای تعدیل درجه کنترل شناختی مورد نیاز برای حفظ رفتار در راستای اهداف فعلی تحت نظر دارد.
The frontal cortex is present in all mammalian species. Evolutionarily speaking, this part of the brain has become much larger in primates relative to other mammals (Figure 12.1). Interestingly, when compared to other primate species, the expansion of prefrontal cortex in the human brain is more pronounced in the white matter (the axonal tracts) than in the gray matter (the cell bodies; Schoenemann et al., 2005). This finding suggests that the cognitive capabilities that are uniquely human may be due to how our brains are connected rather than an increase in the number of neurons.
قشر پیشانی در همه گونههای پستانداران وجود دارد. از نظر تکاملی، این بخش از مغز در پریماتها نسبت به سایر پستانداران بسیار بزرگتر شده است (شکل 12.1). جالب توجه است که در مقایسه با دیگر گونههای پستانداران، گسترش قشر پرهفرونتال در مغز انسان در ماده سفید (مسیرهای آکسون) بیشتر از ماده خاکستری است (اجسام سلولی؛ شوئنمان و همکاران، 2005). این یافته نشان میدهد که تواناییهای شناختی که منحصراً انسانی هستند، ممکن است به دلیل نحوه اتصال مغز ما به جای افزایش تعداد نورونها باشد.
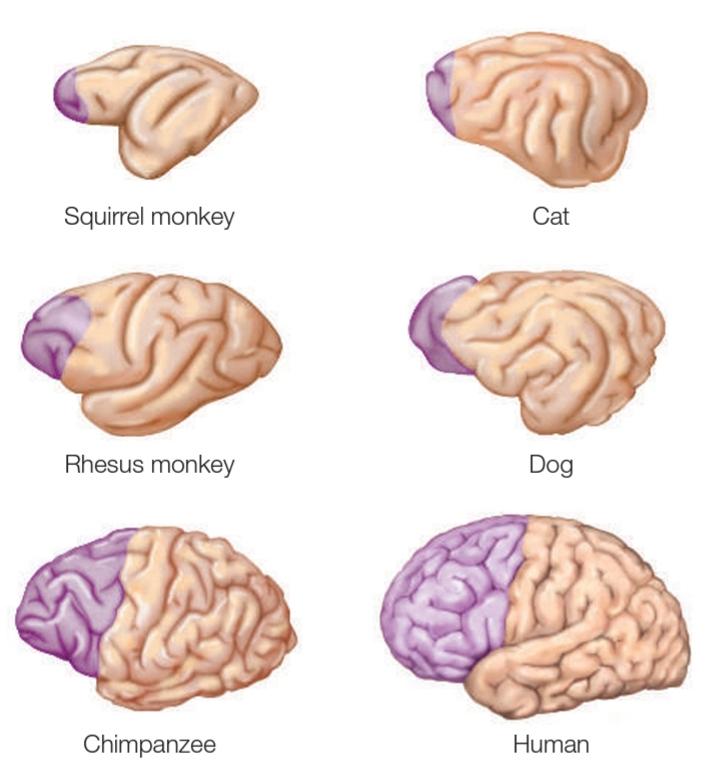
FIGURE 12.1 A comparison of prefrontal cortex in different species. The purple region indicates the PFC in six mammalian species. Although the brains are not drawn to scale, the figure makes clear that the PFC spans a much larger percentage of the overall cortex in the chimpanzee and human.
شکل 12.1 مقایسه قشر پرهفرونتال در گونههای مختلف. ناحیه بنفش نشان دهنده PFC در شش گونه پستاندار است. اگرچه مغزها به مقیاس کشیده نمیشوند، اما این شکل روشن میکند که PFC درصد بسیار بیشتری از قشر کلی در شامپانزه و انسان را در بر میگیرد.
Because the development of functional capabilities parallels phylogenetic trends, the frontal lobe’s expansion is related to the emergence of the complex cognitive capabilities that are especially pronounced in humans. What’s more, as investigators frequently note, “Ontogeny recapitulates phylogeny.” Compared to the rest of the brain, prefrontal cortex matures late, in terms of the development of neural density patterns and white matter tracts. Correspondingly, cognitive control processes appear relatively late in development, as is evident in the “me-oriented” behavior of infants and teenagers.
از آنجایی که توسعه قابلیتهای عملکردی با روندهای فیلوژنتیکی موازی است، گسترش لوب پیشانی به ظهور قابلیتهای شناختی پیچیدهای مرتبط است که بهویژه در انسان برجسته است. علاوه بر این، همانطور که محققان اغلب خاطرنشان میکنند، «رشد فردی تکرارِ رشد گونه ی انسانی است به عبارتی: آنتوژنی، فیلوژنی را تکرار میکند [این امر به نظریه بازپدیدآیی معروف است].» در مقایسه با بقیه مغز، قشر پرهفرونتال از نظر ایجاد الگوهای تراکم عصبی و مسیرهای ماده سفید دیر بالغ میشود. به همین ترتیب، فرآیندهای کنترل شناختی نسبتاً دیر در رشد ظاهر میشوند، همانطور که در رفتار «من محور» نوزادان و نوجوانان مشهود است.
The prefrontal cortex coordinates processing across wide regions of the central nervous system (CNS). It contains a massively connected network that links the brain’s motor, perceptual, and limbic regions (Goldman- Rakic, 1995; Passingham, 1993). Extensive, reciprocal projections connect the prefrontal cortex to almost all regions of the parietal and temporal cortex, and to prestriate regions of the occipital cortex. The PFC also receives a huge input from the thalamus, relaying information from the basal ganglia, cerebellum, and various brainstem nuclei. Indeed, almost all cortical and subcortical areas influence the prefrontal cortex either through direct projections or indirectly via a few synapses. The prefrontal cortex has many projections to the contralateral hemisphere-projections to homologous prefrontal areas via the corpus callosum, as well as bilateral projections to premotor and subcortical regions.
قشر پرهفرونتال پردازش را در مناطق وسیعی از سیستم عصبی مرکزی (CNS) هماهنگ میکند. این شامل یک شبکه انبوه متصل است که نواحی حرکتی، ادراکی و لیمبیک مغز را به هم مرتبط میکند (گلدمن-راکیک، 1995؛ پاسینگهام، 1993). پروجشکنهای دوطرفه گسترده، قشر پرهفرونتال را تقریباً به تمام نواحی قشر آهیانهای و تمپورال و به نواحی پیش از قشر پس سری متصل میکند. PFC همچنین ورودی عظیمیرا از تالاموس دریافت میکند و اطلاعات را از عقدههای قاعدهای، مخچه و هستههای مختلف ساقه مغز منتقل میکند. در واقع، تقریباً تمام نواحی قشری و زیر قشری یا از طریق پروجکشنهای مستقیم یا غیرمستقیم توسط چند سیناپس بر قشر پرهفرونتال تأثیر میگذارند. قشر پرهفرونتال دارای پروجکشنهای زیادی به نیمکره طرف مقابل-پروجکشنها به نواحی همولوگ پیش پیشانی از طریق جسم پینه ای و همچنین پروجکشنهای دوطرفه به نواحی پیش حرکتی و زیر قشری است.
TAKE-HOME MESSAGES
نکات اصلی
▪️ Cognitive control is the collection of mental abilities that involve planning, controlling, and regulating the flow of information processing.
▪️ کنترل شناختی مجموعه ای از تواناییهای ذهنی است که شامل برنامه ریزی، کنترل و تنظیم جریان پردازش اطلاعات است.
▪️ Cognitive control gives us the flexibility required for goal- oriented behavior.
▪️ کنترل شناختی به ما انعطاف لازم برای رفتار هدفمند را میدهد
▪️ The prefrontal cortex includes four major components:
lateral prefrontal cortex, frontal pole, orbitofrontal cortex, and medial frontal cortex. These parts of the brain have become very prominent in mammals, and especially in primates.
▪️ قشر پرهفرونتال شامل چهار جزء اصلی است: قشر پرهفرونتال جانبی، قطب فرونتال، قشر اوربیتوفرونتال و قشر پیشانی داخلی. این قسمتهای مغز در پستانداران و به ویژه در پستانداران بسیار برجسته شده اند.
12.2 Cognitive Control Deficits
12.2 نقص کنترل شناختی
People with frontal lobe lesions-like W.R., the wayward lawyer-present a paradox. From a superficial look at their everyday behavior, it is frequently difficult to detect a neurological disorder: They do not display obvious deficits in any of their perceptual abilities, they can execute motor actions, and their speech is fluent and coherent. They are unimpaired on conventional neuropsychological tests of intelligence and knowledge. They generally score within the normal range on IQ tests. Their memory for previously learned facts is fine, and they do well on most tests of long-term memory. With more sensitive and specific tests, however, it becomes clear that frontal lesions can disrupt different aspects of normal cognition and memory, producing an array of problems.
افراد مبتلا به ضایعات لوب فرونتال مانند دبلیو. آر.، وکیل متعصب، یک پارادوکس را نشان میدهند. از یک نگاه سطحی به رفتار روزمره آنها، تشخیص یک اختلال عصبی اغلب دشوار است: آنها نقص آشکاری در هیچ یک از تواناییهای ادراکی خود نشان نمیدهند، میتوانند اعمال حرکتی را انجام دهند و گفتار آنها روان و منسجم است. آنها در آزمونهای عصبروانشناختی متعارف هوش و دانش آسیبی ندارند. آنها به طور کلی در تستهای IQ در محدوده نرمال نمره میگیرند. حافظه آنها برای حقایقی که قبلاً آموخته اند خوب است و در اکثر تستهای حافظه بلند مدت به خوبی عمل میکنند. با این حال، با آزمایشهای حساستر و خاصتر، مشخص میشود که ضایعات فرونتال میتوانند جنبههای مختلف شناخت و حافظه طبیعی را مختل کنند و مجموعهای از مشکلات را ایجاد کنند.
Such patients may persist in a response even after being told that it is incorrect; this behavior is known as perseveration. They may be apathetic, distractible, or impulsive. They may be unable to make decisions, plan actions, understand the consequences of their actions, organize and segregate the timing of events in memory, remember the source of their memories, and follow rules. They may disregard social conventions (discussed in Chapter 13). Ironically, patients with frontal lobe lesions are aware of their deteriorating social situation, have the intellectual capabilities to generate ideas that may alleviate their problems, and may be able to tell you the pros and cons of each idea. Yet their efforts to prioritize and organize these ideas into a plan and put them into play are haphazard at best. Similarly, although they are not amnesic and can list rules from memory, they may not be able to follow them.
چنین بیمارانی ممکن است حتی پس از اینکه به آنها گفته شود که پاسخ نادرست است، همچنان بر پاسخ خود اصرار ورزند. این رفتار به عنوان تکرار یا درجا زدن شناخته میشود. آنها ممکن است بی تفاوت، حواس پرت یا تکانشی باشند. آنها ممکن است قادر به تصمیم گیری، برنامه ریزی اقدامات، درک پیامدهای اعمال خود، سازماندهی و جداسازی زمان رویدادها در حافظه، به خاطر سپردن منبع خاطرات خود و پیروی از قوانین نباشند. آنها ممکن است قراردادهای اجتماعی را نادیده بگیرند (در فصل 13 مورد بحث قرار میگیرد). عجیب اینکه، بیماران مبتلا به ضایعات لوب فرونتال از وضعیت اجتماعی رو به وخامت خود آگاه هستند، تواناییهای فکری برای ایجاد ایدههایی دارند که ممکن است مشکلات آنها را کاهش دهد، و ممکن است بتوانند جوانب مثبت و منفی هر ایده را به شما بگویند. با این حال، تلاشهای آنها برای اولویتبندی و سازماندهی این ایدهها در یک طرح و اجرای آنها در بهترین حالت تصادفی است. به طور مشابه، اگرچه آنها فراموشی ندارند و میتوانند قوانین را از حافظه فهرست کنند، اما ممکن است نتوانند از آنها پیروی کنند.
To demonstrate how seemingly subtle deficits in cognition may snowball into severe limitations in real-world situations, Tim Shallice of University College London (Shallice & Burgess, 1991) took three patients with frontal lesions to a shopping center, assigning each a short shopping list. Obtaining all the items on the list presented a real problem for the patients. One patient failed to purchase soap because the store she visited did not carry her favorite brand; another wandered outside the desig- nated shopping center in pursuit of an item that could easily be found within the designated region. All became embroiled in social complications. One succeeded in obtaining a newspaper but was pursued by the merchant for failing to pay!
تیم شالیس از دانشگاه کالج لندن (شالیس و برگس، 1991) برای نشان دادن اینکه چگونه نقصهای به ظاهر جزئی در شناخت ممکن است در شرایط دنیای واقعی به محدودیتهای شدید تبدیل شود، سه بیمار مبتلا به ضایعات پیشانی را به یک مرکز خرید برد و به هر یک از آنها یک لیست خرید مختصر اختصاص داد. به دست آوردن تمام موارد موجود در لیست یک مشکل واقعی برای بیماران ایجاد کرد. یکی از بیماران موفق به خرید صابون نشد زیرا فروشگاهی که از آن بازدید کرد مارک مورد علاقه او را نداشت. یکی دیگر به دنبال کالایی که به راحتی در منطقه تعیین شده یافت میشد، خارج از مرکز خرید تعیین شده سرگردان بود. همه درگیر عقدههای اجتماعی شدند. یکی موفق به تهیه روزنامه شد اما به دلیل عدم پرداخت هزینه توسط مغازه دار تحت تعقیب قرار گرفت!
Studies in animals with lesions to their prefrontal cortex revealed behaviors similar to those exhibited by these patients who were unable to complete a plan and were socially inappropriate. Unilateral lesions of prefrontal cortex tend to produce relatively mild deficits in these animals, but dramatic changes can be observed when PFC lesions are extended bilaterally. Consider the obser- vations of Leonardo Bianchi (1922), an Italian psychia- trist of the early 20th century:
مطالعات روی حیوانات با ضایعات قشر پرهفرونتال نشان داد رفتارهایی شبیه به رفتارهایی که این بیماران نشان دادند که قادر به تکمیل یک برنامه نبودند و از نظر اجتماعی نامناسب بودند. ضایعات یک طرفه قشر پرهفرونتال به ایجاد نقص نسبتاً خفیف در این حیوانات منتج میشد، اما هنگامیکه ضایعات PFC به صورت دوطرفه گسترش مییابند، تغییرات چشمگیری قابل مشاهده بود. مشاهدات لئوناردو بیانکی (1922)، روانپزشک ایتالیایی در اوایل قرن بیستم را در نظر بگیرید:
The monkey which used to jump on to the window- ledge, to call out to his companions, after the operation jumps to the ledge again, but does not call out. The sight of the window determines the reflex of the jump, but the purpose is now lacking, for it is no longer represented in the focal point of consciousness…. Another monkey sees the handle of the door and grasps it, but the mental process stops at the sight of the bright colour of the handle. The animal does not attempt to turn it so as to open the door…. Evidently there are lacking all those oth- er images that are necessary for the determination of a series of movements coordinated towards one end.
میمونی که برای صدا زدن همراهانش به لبه پنجره میپرید، بعد از عملیات دوباره به سمت طاقچه میپرد، اما صدا نمیزند. دیدن پنجره بازتاب پرش را مشخص میکند، اما اکنون هدف وجود ندارد، زیرا دیگر در نقطه کانونی آگاهی نشان داده نمیشود… میمون دیگری دستگیره در را میبیند و آن را میگیرد، اما ذهن ذهنی فرآیند با مشاهده رنگ روشن دسته متوقف میشود. حیوان سعی نمیکند آن را بچرخاند تا در را باز کند… بدیهی است که تمام تصاویر دیگری که برای تعیین یک سری حرکات هماهنگ شده به سمت یک انتها ضروری هستند، وجود ندارد.
As with W.R., the monkeys demonstrate a loss of goal-oriented behavior. Indeed, the behavior of these monkeys has become stimulus driven. The animal sees the ledge and jumps up; another sees the door and grasps the handle, but that is the end of it. They no longer appear to have a purpose for their actions. The sight of the door is no longer a sufficient cue to remind the animal of the food and other animals that can be found beyond it.
مانند دبلیو. آر.، میمونها رفتار هدفمحور را از دست میدهند. در واقع، رفتار این میمونها محرک شده است. حیوان طاقچه را میبیند و میپرد. دیگری در را میبیند و دستگیره را میگیرد، اما این پایان کار است. آنها دیگر هدفی برای اعمال خود ندارند. دیدن در دیگر نشانه کافی برای یادآوری غذا و سایر حیواناتی که در ورای آن یافت میشود نیست.
A classic demonstration of this tendency for humans with frontal lobe injuries to exhibit stimulus-driven behavior is evident from the clinical observations of François Lhermitte of the Pitié-Salpêtrière Hospital in Paris (Lhermitte, 1983; Lhermitte et al., 1986). Lher- mitte invited a patient to meet him in his office. At the entrance to the room, he had placed a hammer, a nail, and a picture. Upon entering the room and seeing these objects, the patient spontaneously used the hammer and nail to hang the picture on the wall. In a more extreme example, Lhermitte put a hypodermic needle on his desk, dropped his trousers, and turned his back to his patient. Whereas most people in this situation would consider filing ethical charges, the patient was unfazed. He simply picked up the needle and gave his doctor a healthy jab in the buttocks!
یک نمایش کلاسیک از این تمایل برای انسانهایی که آسیبهای لوب فرونتال دارند برای نشان دادن رفتار محرکمحور از مشاهدات بالینی فرانسوا لرمیت از بیمارستان پیتی-سالپترییر در پاریس مشهود است (لرمیت، 1983; لرمیت و همکاران، 1986). لرمیت یک بیمار را دعوت کرد تا او را در مطب خود ملاقات کند. در ورودی اتاق یک چکش، یک میخ و یک عکس گذاشته بود. بیمار با ورود به اتاق و دیدن این اشیاء، خود به خود با استفاده از چکش و میخ عکس را به دیوار آویزان کرد. در مثال افراطی تر، لرمیت یک سوزن زیرپوستی روی میزش گذاشت، شلوارش را انداخت و پشتش را به بیمارش چرخاند. در حالی که اکثر افراد در این شرایط به بررسی اتهامات اخلاقی میپردازند، بیمار نگران نبود. او به سادگی سوزن را برداشت و به پزشکش یک ضربه سالم به باسن زد!
Lhermitte coined the term utilization behavior to characterize this extreme dependency on prototypical responses for guiding behavior. The patients with frontal lobe damage retained knowledge about prototypical uses of objects such as a hammer or needle, saw the stimulus, and responded. They were not able to inhibit their response or flexibly change it to fit the context in which they found themselves. Their cognitive control mechanisms were out of whack.
لرمیت اصطلاح رفتار استفاده را برای توصیف این وابستگی شدید به پاسخهای اولیه برای هدایت رفتار ابداع کرد. بیماران مبتلا به آسیب لوب فرونتال دانش خود را در مورد استفادههای اولیه از اشیاء مانند چکش یا سوزن حفظ کردند، محرک را دیدند و پاسخ دادند. آنها قادر نبودند از پاسخ خود جلوگیری کنند یا آن را به گونه ای انعطاف پذیر تغییر دهند تا با زمینه ای که در آن قرار گرفته اند مطابقت داشته باشد. مکانیسمهای کنترل شناختی آنها از کار افتاده بود.
Deficits in cognitive control are also considered a hallmark of many psychiatric conditions, including depression, schizophrenia, obsessive-compulsive disorder (OCD), and attention deficit hyperactivity disorder (ADHD; De Zeeuw & Durston, 2017), as well as antisocial personality disorder and psychopathy (Zeier et al., 2012). Even in individuals who do not have clinically defined conditions, impairments in cognitive control become manifest when people experience stress, sadness, loneliness, or poor health (reviewed in Diamond & Ling, 2016).
نقص در کنترل شناختی نیز یکی از مشخصههای بارز بسیاری از بیماریهای روانپزشکی، از جمله افسردگی، اسکیزوفرنی، اختلال وسواس فکری-اجباری (OCD) و اختلال نقص توجه بیشفعالی (ADHD؛ د زیو و درستون، 2017) و همچنین اختلال شخصیت ضد اجتماعی و روانپریشی (زیر و همکاران، 2012). حتی در افرادی که شرایط بالینی تعریف شده ندارند، اختلالات در کنترل شناختی زمانی آشکار میشود که افراد استرس، غم، تنهایی یا سلامت ضعیف را تجربه میکنند (بازبینی در دیاموند و لینگ، 2016).
A hallmark of drug or alcohol addiction is the sense of a loss of control. One model of drug addiction suggests that disruption of PFC function underlies the characteristic problems addicts have in inhibiting destructive behaviors and appropriately evaluating the relevance of behavioral cues (Goldstein & Volkow, 2011). Hugh Garavan and colleagues at Trinity College in Ireland conducted a series of studies to ask whether the cognitive control changes that occur in cocaine users would also manifest in the lab (Kaufman et al., 2003). In one task, the participants viewed a stream of stimuli that alter- nated between two letters and were instructed to quickly press a button with the presentation of each letter. In rare instances, however, the same letter was repeated on suc- cessive trials. For these “no-go” trials, participants were instructed to withhold their response.
یکی از مشخصههای اعتیاد به مواد مخدر یا الکل، احساس از دست دادن کنترل است. یک مدل از اعتیاد به مواد مخدر نشان میدهد که اختلال در عملکرد PFC زمینه ساز مشکلات مشخصه ای است که معتادان در مهار رفتارهای مخرب و ارزیابی مناسب ارتباط نشانههای رفتاری دارند (گلدشتاین و ولکو، 2011). هیو گاراوان و همکارانش در کالج ترینیتی در ایرلند، مجموعه ای از مطالعات را انجام دادند تا بپرسند آیا تغییرات کنترل شناختی که در مصرف کنندگان کوکائین رخ میدهد، در آزمایشگاه نیز آشکار میشود (کافمن و همکاران، 2003). در یک کار، شرکتکنندگان جریانی از محرکها را مشاهده کردند که بین دو حرف تغییر میکرد و به آنها دستور داده شد که به سرعت یک دکمه را با ارائه هر حرف فشار دهند. با این حال، در موارد نادری، همان نامه در آزمایشهای متوالی تکرار میشد. برای این کارآزماییهای «ممنوع»، به شرکتکنندگان دستور داده شد که از پاسخ خودداری کنند.
Chronic cocaine users, none of whom had used cocaine for 18 hours before testing, were more likely to respond on the no-go trials than were matched controls—a result that was interpreted as evidence of a general problem with response inhibition. The cocaine users also showed lower activation in the medial frontal cortex when they produced these erroneous responses. As we will see later in this chapter, this pattern suggests that they had difficulty monitoring their performance. Thus, even when the drug users were not under the influence of cocaine and were not making choices related to their addiction, changes in cognitive control persisted.
مصرف کنندگان مزمن کوکائین، که هیچ یک از آنها به مدت 18 ساعت قبل از آزمایش کوکائین مصرف نکرده بودند، در کارآزماییهای ممنوعه نسبت به گروه کنترل همسان بیشتر احتمال داشت پاسخ دهند – نتیجه ای که به عنوان شواهدی از یک مشکل کلی در مهار پاسخ تفسیر شد. مصرف كنندگان كوكائين همچنين فعاليت كمتري را در قشر فرونتال داخلي نشان دادند كه اين پاسخهاي اشتباه را ايجاد كردند. همانطور که در ادامه این فصل خواهیم دید، این الگو نشان میدهد که آنها در نظارت بر عملکرد خود مشکل داشتند. بنابراین، حتی زمانی که مصرفکنندگان مواد تحت تأثیر کوکائین نبودند و انتخابهای مرتبط با اعتیاد خود را انجام نمیدادند، تغییرات در کنترل شناختی ادامه داشت.
TAKE-HOME MESSAGES
نکات اصلی
▪️Patients with frontal lobe lesions have difficulty executing a plan and may exhibit stimulus-driven behavior.
▪️ بیماران مبتلا به ضایعات لوب فرونتال در اجرای طرح مشکل دارند و ممکن است رفتار محرکی از خود نشان دهند.
▪️Deficits in cognitive control are found in numerous psychiatric disorders, as well as when mental health is compromised by situational factors such as stress or loneliness.
▪️نقص در کنترل شناختی در بسیاری از اختلالات روانپزشکی و همچنین زمانی که سلامت روان توسط عوامل موقعیتی مانند استرس یا تنهایی به خطر میافتد، دیده میشود.

 ورود/ ثبت نام با جیمیل
ورود/ ثبت نام با جیمیل
