
ترجمه و بازنویسی علمی فصول کتاب «نوروآناتومی بالینی» | کتاب درسی جامع ساختارهای عصبی (ویرایش دوم)
کتاب درسی نوروآناتومی بالینی، ویرایش دوم. Textbook of Clinical Neuroanatomy (2nd ed.) یکی از منابع معتبر در حوزه نوروآناتومی بالینی (Clinical Neuroanatomy) است که با رویکردی کاربردی، ساختارها و مسیرهای سیستم عصبی (Nervous System) را بهصورت نظاممند و بالینی شرح میدهد.
این ترجمه آموزشی، حاصل تلاش تیم علمی آیندهنگاران مغز به سرپرستی داریوش طاهری است و با هدف ارتقای آموزش علوم اعصاب (Neuroscience) در زبان فارسی، با حفظ دقت علمی، به زبانی روان تدوین شده است.
در ۲۰ فصل این مجموعه، ساختارهایی چون مغز (Brain)، نخاع (Spinal Cord)، اعصاب مغزی (Cranial Nerves)، سیستم لیمبیک (Limbic System)، مسیرهای حسی و حرکتی (Sensory and Motor Pathways)، مخچه (Cerebellum)، دیانسفالون (Diencephalon) و سیستم عصبی خودمختار (Autonomic Nervous System) بررسی میشوند.
این مجموعه برای دانشجویان پزشکی، رزیدنتها و متخصصان علاقهمند به نوروساینس بالینی طراحی شده و تلفیقی از مفاهیم بنیادی، نکات بالینی و نمودارهای عملکردی را ارائه میدهد.
با سپاس از همراهی شما
تیم آیندهنگاران مغز | سرپرستی: داریوش طاهری
16. Meninges And Cerebrospinal Fluid
۱۶. مننژ و مایع مغزی نخاعی
Meninges
The brain and spinal cord are enclosed in three protective membranes called meninges. From without inwards these are: (a) dura mater, (b) arachnoid mater, and (c) pia mater.
مننژ
مغز و نخاع در سه غشای محافظ به نام مننژ محصور شدهاند. از بیرون به داخل عبارتند از: (الف) سختشامه، (ب) عنکبوتیه، و (ج) نرمشامه.
The dura mater is mesodermal in origin while arachnoid and pia mater are ectodermal in origin (derived from neural crests).
سختشامه منشأ مزودرمی دارد در حالی که عنکبوتیه و نرمشامه منشأ اکتودرمی دارند (از ستیغهای عصبی مشتق شدهاند).
The dura mater is the thick outermost covering of the brain and spinal cord. The part enclosing the brain is called cranial/cerebral dura, and the part around the spinal cord, the spinal dura. It is very tough opaque inelastic membrane of fibrous tissue (Gk. dura = tough, mater = mother). It is also called pachymeninx (pachy = thick).
سختشامه بیرونیترین پوشش ضخیم مغز و نخاع است. بخشی که مغز را در بر میگیرد، سختشامه جمجمهای/مغزی و بخشی که نخاع را احاطه کرده، سختشامه نخاعی نامیده میشود. این غشای بسیار سخت و مات و غیرالاستیک از بافت فیبری است (سختشامه = سفت، ماده = مادر). همچنین پاکیمنینکس (پاکی = ضخیم) نامیده میشود.
The arachnoid mater (Gk. arachnoid = cobweb like, mater = mother) is a delicate avascular membrane deep to dura mater. Many thread-like trabeculae extend from it to the pia mater.
عنکبوتیه (عنکبوتیه = تار عنکبوت مانند، ماده = مادر) یک غشای ظریف بدون رگ در عمق سختشامه است. بسیاری از ترابکولهای نخمانند از آن تا نرمشامه امتداد دارند.
The pia mater (Gk. pia = tender, mater = mother) is a thin transparent vascular membrane closely adherent to the surface of the brain and spinal cord.
نرمشامه (به زبان یونانی pia = نرمشامه، mater = مادر) یک غشای عروقی نازک و شفاف است که به سطح مغز و نخاع چسبیده است.
The arachnoid mater and pia mater together are termed leptomeninges (Gk. lepto = thin).
نرمشامه و نرمشامه با هم لپتومننژ (به زبان یونانی lepto = نازک) نامیده میشوند.
The intracranial arrangement of these membranes differs from that in the vertebral canal and are therefore described separately.
ترتیب قرارگیری داخل جمجمهای این غشاها با ترتیب قرارگیری آنها در کانال مهرهای متفاوت است و بنابراین جداگانه شرح داده میشوند.
The spinal meninges are described in Chapter 7).
مننژهای نخاعی در فصل 7 شرح داده شدهاند.
Intracranial Meninges
Dura mater
The dura mater in the cranium (cranial dura) consists of two layers: an outer endosteal layer and an inner meningeal layer. These two layers are firmly adherent to each other everywhere except, (a) where they split to enclose the venous sinuses, and (b) where the inner layer is folded to form the dural septa.
مننژ داخل جمجمهای
سختشامه
سختشامه در جمجمه (سختشامه جمجمهای) از دو لایه تشکیل شده است: یک لایه اندوستئال خارجی و یک لایه مننژئال داخلی. این دو لایه در همه جا به جز (الف) جایی که برای محصور کردن سینوسهای وریدی از هم جدا میشوند، و (ب) جایی که لایه داخلی برای تشکیل دیواره سختشامه تا میشود، محکم به یکدیگر چسبیدهاند.
The endosteal layer is attached to the inner surfaces of the cranial bones and is continuous through the sutural ligaments, and around the margins of the foramina with the periosteum on the external surface of the cranium.
لایه اندوستئال به سطوح داخلی استخوانهای جمجمه متصل است و از طریق رباطهای بخیهای و در اطراف حاشیههای سوراخها با پریوستئوم روی سطح خارجی جمجمه پیوسته است.
Clinical Correlation
The cranial dura is more firmly adherent to the base of skull than on the vault, hence, usually torn in fractures of the skull base. It also forms the part of the wall of the basal venous sinuses, hence the fractures of skull base are often associated with bleeding from ear, nose, or into the pharynx. Cerebral dura is usually stripped off from the cranial vault, when an extradural haematoma is formed between the bone and dura.
همبستگی بالینی
سختشامه جمجمهای نسبت به طاق جمجمه، محکمتر به قاعده جمجمه میچسبد، از این رو، معمولاً در شکستگیهای قاعده جمجمه پاره میشود. همچنین بخشی از دیواره سینوسهای وریدی قاعده جمجمه را تشکیل میدهد، از این رو شکستگیهای قاعده جمجمه اغلب با خونریزی از گوش، بینی یا حلق همراه است. سختشامه مغزی معمولاً از طاق جمجمه جدا میشود، زمانی که هماتوم خارج سختشامه بین استخوان و سختشامه تشکیل میشود.
The meningeal layer is a strong fibrous membrane and becomes continuous with the spinal dura at the foramen magnum. It ensheathes the cranial nerves in their osseous foramina and fuses externally with epineurium; the sheaths of the optic nerves fuse with the ocular sclera.
لایه مننژ یک غشای فیبری قوی است و در سوراخ بزرگ به سختشامه نخاعی متصل میشود. این لایه، اعصاب جمجمهای را در سوراخهای استخوانیشان میپوشاند و از خارج با اپینوریوم ترکیب میشود. غلافهای اعصاب بینایی با صلبیه چشم ترکیب میشوند.
Dura! septa or folds (Figs 16.1, 16.2)
The meningeal layer gets reduplicated (infolded) along certain lines and forms septa or folds between the parts of the brain.
دیوارهها یا چینهای سختشامه (شکلهای ۱۶.۱، ۱۶.۲)
لایه مننژ در امتداد خطوط خاصی دوباره تکثیر (چینخوردگی) میشود و دیوارهها یا چینهایی را بین قسمتهای مغز تشکیل میدهد.
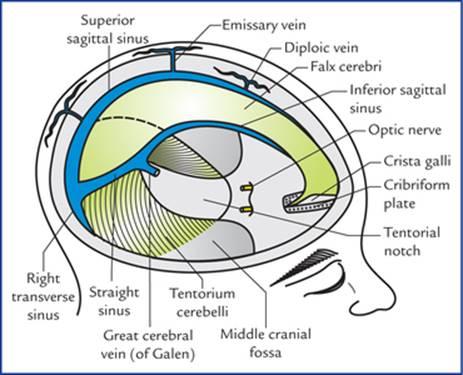
FIG. 16.1 Dural septa and dural venous sinuses viewed from superolateral aspect.
شکل 16.1 دیواره سختشامه و سینوسهای وریدی سختشامه از نمای فوقانی-جانبی.
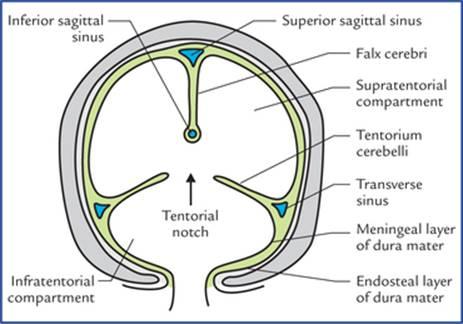
FIG. 16.2 Schematic coronal section of skull showing division of cranial cavity into three compartments by falx cerebri and tentorium cerebelli. Each half of the supratentorial compartment contains the cerebral hemisphere, whereas the infratentorial compartment contains the cerebellum and brainstem.
شکل 16.2 برش شماتیک تاجی جمجمه که تقسیم حفره جمجمه به سه بخش توسط داس مغزی و چادرینه مخچه را نشان میدهد. هر نیمه از بخش بالای چادرینه شامل نیمکره مغزی است، در حالی که بخش زیر چادرینه شامل مخچه و ساقه مغز است.
The four important dural septa are:
1. Falx cerebri
2. Falx cerebelli
3. Tentorium cerebelli
4. Diaphragma sellae.
چهار سپتوم مهم دورال عبارتند از:
۱. داس مغزی
۲. داس مخچه
۳. چادرینه مخچه
۴. دیافراگم زین ترکی
Functions of dural septa
1. Dural septa divide the cranial cavity into compartments to separate the different parts of the brain and thus restrict their movements within the cranial cavity (Fig. 16.1).
2. They enclose intracranial dural venous sinuses.
وظایف دیوارههای سختشامه
1. دیوارههای سختشامه حفره جمجمه را به بخشهایی تقسیم میکنند تا قسمتهای مختلف مغز را از هم جدا کرده و در نتیجه حرکات آنها را در حفره جمجمه محدود کنند (شکل 16.1).
2. آنها سینوسهای وریدی سختشامه داخل جمجمهای را محصور میکنند.
Falx Cerebri
Falx cerebri is a large sickle-shaped vertical fold of dura mater which dips into the longitudinal fissure, between the two cerebral hemispheres.
داس مغزی
داس مغزی یک چین عمودی بزرگ داسی شکل از سخت شامه است که در شکاف طولی بین دو نیمکره مغزی فرو میرود.
Its narrow anterior end is attached to the crista galli and its broad posterior end to the upper surface of the tentorium cerebelli. Its convex upper border is attached to the vault of skull along the sagittal suture and its lower border is free and concave downwards.
انتهای قدامی باریک آن به کریستا گالی و انتهای خلفی پهن آن به سطح فوقانی چادرینه مخچه متصل است. لبه بالایی محدب آن در امتداد درز ساژیتال به طاق جمجمه متصل است و لبه پایینی آن آزاد و به سمت پایین مقعر است.
The falx cerebri encloses three dural venous sinuses, viz.
• Superior sagittal sinus, along its upper attached border.
• Inferior sagittal sinus, along its lower free border.
• Straight sinus, along its line of attachment with the tentorium cerebelli.
داس مغزی سه سینوس وریدی سختشامه را در بر میگیرد، که عبارتند از:
• سینوس ساژیتال فوقانی، در امتداد لبه متصل فوقانی آن.
• سینوس ساژیتال تحتانی، در امتداد لبه آزاد تحتانی آن.
• سینوس مستقیم، در امتداد خط اتصال آن با چادرینه مخچه.
Tentorium cerebelli
Tentorium cerebelli is tent-like semilunar fold of dura mater which forms the sloping roof of the posterior cranial fossa, between the cerebellum below and the occipital lobes of cerebral hemispheres above. It prevents the cerebellum from being compressed by the heavy cerebrum.
چادرینه مخچه
چادر مخچه چین نیمه هلالی چادر مانندی از سخت شامه است که سقف شیبدار حفره جمجمهای خلفی، بین مخچه در پایین و لوبهای پسسری نیمکرههای مغزی در بالا را تشکیل میدهد. این چین از فشرده شدن مخچه توسط مخ سنگین جلوگیری میکند.
It has two borders: (a) an outer convex attached border, and (b) an inner concave free border. The inner border bounds an oval space, the tentorial notch or the door of tentorium through which passes the midbrain to connect the hindbrain with the forebrain (Fig. 16.2).
این چادر دارای دو لبه است: (الف) یک لبه بیرونی محدب متصل، و (ب) یک لبه داخلی مقعر آزاد. لبه داخلی یک فضای بیضی شکل، بریدگی چادری یا درب چادرینه را محدود میکند که از طریق آن مغز میانی عبور میکند تا مغز خلفی را به مغز قدامی متصل کند (شکل 16.2).
On each side, the anterior half of the outer border is attached anterolaterally to the superior border of the petrous temporal bone and posterior clinoid process, and posterior half is attached posterolaterally to the lips of the transverse sulcus.
در هر طرف، نیمه قدامی لبه بیرونی به صورت قدامی-خارجی به لبه فوقانی استخوان گیجگاهی خارهای و زائده کلینوئید خلفی متصل است و نیمه خلفی به صورت خلفی-خارجی به لبهای شیار عرضی متصل است.
The inner free border is ‘U’-shaped and its anterior ends are attached to the anterior clinoid processes.
حاشیه آزاد داخلی به شکل U است و انتهای قدامی آن به زوائد کلینوئید قدامی متصل است.
Tentorium cerebelli contains four dural venous sinuses, two on either side:
• Superior petrosal sinus, along the anterior half of its attached border.
• Transverse sinus, along the posterior half of its attached border.
چادرینه مخچه شامل چهار سینوس وریدی سختشامه است که دو عدد در دو طرف آن قرار دارند:
• سینوس سنگی فوقانی، در امتداد نیمه قدامی لبه متصل آن.
• سینوس عرضی، در امتداد نیمه خلفی لبه متصل آن.
Falx cerebelli
Falx cerebelli is a small sickle-shaped fold of dura mater which intervenes between the two cerebellar hemispheres posteriorly. It is attached to the internal occipital crest by its outer border, and encloses the occipital venous sinus.
داس مخچه
داس مخچه یک چین کوچک داسی شکل از سخت شامه است که از عقب بین دو نیمکره مخچه قرار دارد. این چین توسط لبه بیرونی خود به ستیغ داخلی پس سری متصل است و سینوس وریدی پس سری را در بر میگیرد.
Diaphragma sellae (or tentorium hypophysii)
Diaphragma sellae is a small circular fold of dura mater which roofs the pituitary fossa/sella turcica. It has an aperture in its centre to provide passage for the stalk of the pituitary gland.
دیافراگم سلا (یا چادرینه هیپوفیز)
دیافراگم سلا یک چین دایرهای کوچک از سخت شامه است که حفره هیپوفیز/سلا تورسیکا را میپوشاند. در مرکز خود روزنهای دارد که مسیر ساقه غده هیپوفیز را فراهم میکند.
Arterial supply of dura mater
The dura is supplied by numerous branches of the internal carotid, ascending pharyngeal, maxillary, occipital and vertebral arteries.
خونرسانی شریانی سخت شامه
سخت شامه توسط شاخههای متعددی از شریانهای کاروتید داخلی، حلقی صعودی، فکی، پسسری و مهرهای خونرسانی میشود.
N.B. Middle meningeal artery is the largest of the meningeal arteries and from clinical point of view is the most important for it is often damaged in head injuries.
توجه: شریان مننژیال میانی بزرگترین شریان مننژیال است و از نظر بالینی مهمترین آنهاست زیرا اغلب در آسیبهای سر آسیب میبیند.
Clinical Correlation
The middle meningeal artery, a branch of maxillary artery enters the cranial cavity through the foramen spinosum to lie between the endosteal and meningeal layers of dura mater. Its anterior and posterior branches, along with accompanying meningeal veins (between the arteries and bone) stand out prominently as if in relief on the external surface of the dura mater to groove and supply bones of the cranial vault. The anterior (frontal) branch crosses the pterion, on its inner aspect and the posterior (parietal) branch ascends backwards towards the lambda. A fracture of thin squamous temporal bone may cause a middle meningeal haemorrhage from the artery or vein, producing an extradural haematoma.
همبستگی بالینی
شریان مننژیال میانی، شاخهای از شریان فک بالا، از طریق سوراخ خاری وارد حفره جمجمه میشود تا بین لایههای اندوستئال و مننژیال سختشامه قرار گیرد. شاخههای قدامی و خلفی آن، همراه با رگهای مننژیال همراه (بین شریانها و استخوان) به طور برجستهای، گویی به صورت برجسته روی سطح خارجی سختشامه قرار گرفتهاند تا شیار ایجاد کرده و استخوانهای طاق جمجمه را تغذیه کنند. شاخه قدامی (فرونتال) از پتریون، در قسمت داخلی آن عبور میکند و شاخه خلفی (جداری) به سمت عقب به سمت لامبدا صعود میکند. شکستگی استخوان تمپورال اسکواموس نازک ممکن است باعث خونریزی مننژیال میانی از شریان یا ورید شود و هماتوم خارج سختشامه ایجاد کند.
Nerve supply of dura mater
The nerve supply of dura mater is derived mainly from three sources:
تغذیه عصبی سختشامه
تغذیه عصبی سختشامه عمدتاً از سه منبع تأمین میشود:
1. Three divisions of trigeminal nerve
2. First three cervical spinal nerves
3. Cervical sympathetic trunk.
۱. سه شاخه عصب سه قلو
۲. سه عصب اول نخاعی گردنی
۳. تنه سمپاتیک گردنی.
• The supratentorial dura is supplied by the meningeal branches from the three divisions of the trigeminal nerve:
1. In the anterior cranial fossa by meningeal branches of the anterior and posterior ethmoidal nerves.
2. In the middle cranial fossa by meningeal branches of maxillary and mandibular nerves.
• سخت شامه سوپراتنتوریال توسط شاخههای مننژیال از سه شاخه عصب سه قلو خونرسانی میشود:
۱. در حفره جمجمهای قدامی توسط شاخههای مننژیال اعصاب اتموئیدال قدامی و خلفی.
۲. در حفره جمجمهای میانی توسط شاخههای مننژیال اعصاب فک بالا و پایین.
• The infratentorial dura is supplied by ascending meningeal branches of upper three cervical nerves.
• سختشامه زیر چادرینه توسط شاخههای مننژیال صعودی سه عصب گردنی فوقانی عصبدهی میشود.
Clinical Correlation
The stimulation of sensory nerve endings in the dura mater due to stretching causes pain and is the basis of certain forms of headache. Pain arising from supratentorial dura is referred to the forehead while pain arising from infratentorial dura is referred to the back of the neck and occiput. The role of the autonomic supply of the cranial dura mater is uncertain.
همبستگی بالینی
تحریک انتهای اعصاب حسی در سخت شامه به دلیل کشش باعث درد میشود و اساس انواع خاصی از سردرد است. درد ناشی از سخت شامه سوپراتنتوریال به پیشانی ارجاع داده میشود در حالی که درد ناشی از سخت شامه اینفراتنتوریال به پشت گردن و پس سر ارجاع داده میشود. نقش عصبدهی خودکار سخت شامه جمجمهای نامشخص است.
N.B. The brain itself, the arachnoid mater, and the pia mater do not have sensory nerve endings. These are restricted only to the dura mater and cerebral vessels.
توجه: خود مغز، عنکبوتیه و نرم شامه انتهای اعصاب حسی ندارند. این عصبها فقط به سخت شامه و عروق مغزی محدود میشوند.
Dural venous sinuses
The dural venous sinuses are formed in following two ways: (a) by separation of the two layers of cerebral dura, and (b) by reduplication of the meningeal layer of dura (Fig. 16.2).
سینوسهای وریدی سختشامه
سینوسهای وریدی سختشامه به دو روش زیر تشکیل میشوند: (الف) با جدا شدن دو لایه سختشامه مغزی، و (ب) با تکثیر لایه مننژی سختشامه (شکل 16.2).
The dural venous sinuses are lined by endothelium which becomes continuous with the endothelial lining of the veins.
سینوسهای وریدی سختشامه توسط اندوتلیوم پوشیده شدهاند که با پوشش اندوتلیال وریدها در امتداد قرار میگیرد.
Characteristic features
• Have no valves, hence the blood can flow in either direction in the sinuses,
• Are devoid of smooth muscle fibres in their walls,
• Drain finally into the internal jugular veins,
• Have cerebral, diploic and some meningeal veins as their tributaries,
• Communicate via valveless emissary veins with the extracranial veins through skull foramina.
ویژگیهای مشخصه
• دریچه ندارند، از این رو خون میتواند در هر دو جهت در سینوسها جریان یابد،
• فاقد فیبرهای عضلانی صاف در دیوارههای خود هستند،
• در نهایت به وریدهای ژوگولار داخلی تخلیه میشوند،
• دارای وریدهای مغزی، دیپلوئیک و برخی وریدهای مننژی به عنوان شاخههای فرعی خود هستند،
• از طریق وریدهای فرستنده بدون دریچه از طریق سوراخهای جمجمه با وریدهای خارج جمجمهای ارتباط برقرار میکنند.
Classification
The dural venous sinuses are classified into two types, unpaired and paired (Table 16.1).
طبقهبندی
سینوسهای وریدی سختشامه به دو نوع جفت نشده و جفت شده طبقهبندی میشوند (جدول 16.1).
Table 16.1
Classification of dural venous sinuses
جدول ۱۶.۱
طبقهبندی سینوسهای وریدی سختشامه
Unpaired | Paired |
• Superior sagittal sinus | • Sphenoparietal sinuses |
• Inferior sagittal sinus | • Cavernous sinuses |
• Straight sinus | • Superior petrosal sinuses |
• Occipital sinus | • Inferior petrosal sinuses |
• Anterior intercavernous sinus | • Transverse sinuses |
• Posterior intercavernous sinus | • Sigmoid sinuses |
Unpaired sinuses
Superior sagittal sinus (SSS)
Superior sagittal sinus lies in the attached border of the falx cerebri and extends anteroposteriorly from the foramen caecum where it communicates with the nasal veins to the internal occipital protuberance, where it usually turns to the right side to continue as the right transverse sinus.
سینوسهای جفت نشده
سینوس ساژیتال فوقانی (SSS)
سینوس ساژیتال فوقانی در حاشیه متصل به داس مغزی قرار دارد و از سوراخ سکوم به صورت قدامی-خلفی امتداد مییابد، جایی که با وریدهای بینی تا برآمدگی داخلی پسسری ارتباط برقرار میکند، جایی که معمولاً به سمت راست میچرخد تا به عنوان سینوس عرضی راست ادامه یابد.
Large clusters of arachnoid villi (arachnoid granulations), concerned with the absorption of CSF project into the venous lacunae of the SSS (the clefts between the two layers of dura mater along side the SSS).
خوشههای بزرگی از پرزهای عنکبوتیه (گرانولاسیونهای عنکبوتیه)، که مربوط به جذب CSF هستند، به داخل لاکونهای وریدی SSS (شکافهای بین دو لایه سختشامه در امتداد SSS) پرتاب میشوند.
The 8 to 12 superior cerebral veins ascend with slight anterior inclination, and traverse the subdural space to drain into the superior sagittal sinus and its lacunae.
8 تا 12 ورید مغزی فوقانی با کمی شیب قدامی بالا میروند و از فضای سابدورال عبور میکنند تا به سینوس ساژیتال فوقانی و لاکونهای آن تخلیه شوند.
Clinical Correlation
The superior sagittal sinus communicates with the veins of scalp, diploic veins and sometimes with the veins of the nose. As a result the infection from these areas can spread to the sinus producing thrombosis of superior sagittal sinus.
همبستگی بالینی
سینوس ساژیتال فوقانی با رگهای پوست سر، رگهای دیپلوئیک و گاهی اوقات با رگهای بینی ارتباط دارد. در نتیجه، عفونت از این نواحی میتواند به سینوس گسترش یابد و باعث ترومبوز سینوس ساژیتال فوقانی شود.
Inferior sagittal sinus
Inferior sagittal sinus lies in the posterior two-third of the lower free border of falx cerebri and receives the veins from the medial surfaces of the cerebral hemispheres. At the junction of falx cerebri with the tentorium cerebelli, it is joined by the great cerebral vein to form the straight sinus.
سینوس ساژیتال تحتانی
سینوس ساژیتال تحتانی در دو سوم خلفی لبه آزاد تحتانی داس مغزی قرار دارد و رگهای سطوح داخلی نیمکرههای مغزی را دریافت میکند. در محل اتصال داس مغزی به چادرینه مخچه، توسط ورید بزرگ مغزی به آن متصل میشود و سینوس مستقیم را تشکیل میدهد.
Straight sinus
Straight sinus runs along the line of attachment of falx cerebri with the tentorium cerebelli. At the external occipital protuberance it usually turns to the left to continue as the left transverse sinus.
سینوس مستقیم
سینوس مستقیم در امتداد خط اتصال داس مغزی به چادرینه مخچه امتداد دارد. در برآمدگی پس سری خارجی، معمولاً به سمت چپ میچرخد تا به عنوان سینوس عرضی چپ ادامه یابد.
Occipital sinus
Occipital sinus is the smallest sinus and situated along the attached margin of the falx cerebelli. It extends downwards from the confluence of the sinuses to the foramen magnum, where it communicates with the internal vertebral venous plexus.
سینوس پسسری
سینوس پسسری کوچکترین سینوس است و در امتداد لبه متصل به داس مخچه قرار دارد. این سینوس از محل تلاقی سینوسها به سمت پایین تا سوراخ بزرگ امتداد مییابد، جایی که با شبکه وریدی مهرهای داخلی ارتباط برقرار میکند.
N.B. At the external occipital protuberance the superior sagittal sinus communicates with the left transverse, occipital and straight sinuses to form, what is termed confluence of sinuses.
توجه: در برآمدگی پسسری خارجی، سینوس ساژیتال فوقانی با سینوسهای عرضی چپ، پسسری و مستقیم ارتباط برقرار میکند تا چیزی را تشکیل دهد که به آن “محل تلاقی سینوسها” میگویند.
The shapes of various dural folds, and sinuses enclosed in them are summarized in Table 16.2.
شکل چینهای مختلف سختشامه و سینوسهای محصور در آنها در جدول 16.2 خلاصه شده است.
Table 16.2
Shapes of dural folds and enclosed venous sinuses
جدول 16.2
شکل چینهای سختشامه و سینوسهای وریدی محصور
Fold | Shape | Venous sinuses enclosed |
Falx cerebri | Sickle-shaped | Superior sagittal, inferior sagittal and straight sinuses |
Tentorium cerebelli | Tent-shaped (semilunar) | Transverse and superior petrosal sinuses |
Falx cerebelli | Sickle-shaped | Occipital sinus |
Diaphragma sellae | Horizontal fold | Anterior and posterior intercavernous sinuses |
Paired sinuses
Sphenoparietal sinuses (Fig. 16.4)
These small sinuses lie along the lesser wing of sphenoid and drain into the cavernous sinus.
سینوسهای جفت
سینوسهای اسفنوپاریتال (شکل ۱۶.۴)
این سینوسهای کوچک در امتداد بال کوچک اسفنوئید قرار دارند و به سینوس کاورنوس تخلیه میشوند.
Cavernous sinuses (Figs 16.3, 16.4)
Cavernous sinuses are situated one on either side of the sella turcica and, the body of sphenoid. Each sinus is a short wide venous channel measuring 2 cm anteroposteriorly and 1 cm transversely. It extends from superior orbital fissure anteriorly to the apex of petrous temporal bone posteriorly. The cavernous sinus is so named because it is traversed by a network of trabeculae which subdivide the cavity into numerous communicating caverns lined by endothelium. The two sinuses communicate with each other through anterior and posterior inter-cavernous sinuses which lie in the anterior and posterior margins of the diaphragma sellae, and pass anterior and posterior to the stalk of the pituitary gland respectively.
سینوسهای غاری (شکلهای ۱۶.۳، ۱۶.۴)
سینوسهای غاری در دو طرف زین ترکی و بدنه استخوان اسفنوئید قرار دارند. هر سینوس یک کانال وریدی کوتاه و پهن است که ۲ سانتیمتر در جلو و ۱ سانتیمتر در عرض آن اندازه گیری شده است. این سینوس از شکاف کاسه چشم فوقانی در جلو تا رأس استخوان گیجگاهی خارهای در عقب امتداد دارد. سینوس غاری به این دلیل به این نام خوانده میشود که توسط شبکهای از ترابکولها عبور میکند که حفره را به غارهای ارتباطی متعددی که توسط اندوتلیوم پوشیده شدهاند، تقسیم میکنند. این دو سینوس از طریق سینوسهای بین غاری قدامی و خلفی که در لبههای قدامی و خلفی زین دیافراگم قرار دارند و به ترتیب از جلو و عقب به ساقه غده هیپوفیز میروند، با یکدیگر ارتباط برقرار میکنند.
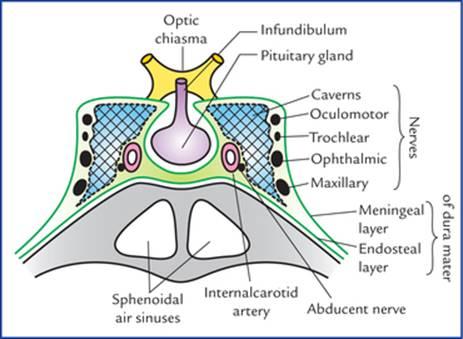
FIG. 16.3 Coronal section of cavernous sinus showing its relations and contents.
شکل ۱۶.۳ برش کرونال سینوس کاورنوس که روابط و محتویات آن را نشان میدهد.

FIG. 16.4 Tributaries and communications of the cavernous sinus. (V = foramen of Vesalius, O = foramen ovale, L = foramen lacerum.)
شکل ۱۶.۴ شاخهها و ارتباطات سینوس کاورنوس. (V = سوراخ وزالیوس، O = سوراخ بیضی، L = سوراخ توری.)
The cavernous and intercavernous sinuses together constitute the circulus sinus.
سینوسهای کاورنوس و بین کاورنوس با هم سینوس سیرکولوس را تشکیل میدهند.
Formation It is formed by the separation of meningeal and endosteal layers of dura mater so that its roof, lateral and medial walls consists of meningeal layer, and its floor consists of endosteal layer. The sinus is filled with venous blood and is covered with an endothelial lining.
تشکیل آن از جداسازی لایههای مننژی و اندوستئال سختشامه تشکیل میشود، به طوری که سقف، دیوارههای جانبی و داخلی آن از لایه مننژی و کف آن از لایه اندوستئال تشکیل شده است. سینوس پر از خون وریدی است و با یک پوشش اندوتلیال پوشیده شده است.
Relations Medially: Pituitary gland and body of sphenoid containing sphenoidal air sinuses.
روابط در قسمت داخلی: غده هیپوفیز و بدنه اسفنوئید حاوی سینوسهای هوایی اسفنوئیدی.
Laterally: Uncus of temporal lobe of brain and trigeminal ganglion lying within the cavum trigeminale.
در قسمت خارجی: آنکوس لوب گیجگاهی مغز و گانگلیون سه قلو که در داخل حفره سه قلو قرار دارد.
Superiorly: Upper limb of the U-shaped loop of internal carotid artery forming carotid siphon.
در قسمت فوقانی: اندام فوقانی حلقه U شکل شریان کاروتید داخلی که سیفون کاروتید را تشکیل میدهد.
Inferiorly: Greater wing of sphenoid.
در قسمت تحتانی: بال بزرگ اسفنوئید.
Each sinus is traversed by an internal carotid artery with sympathetic plexus around it, and abducent nerve, covered by an endothelium. The abducent nerve is inferolateral in relation to the artery.
هر سینوس توسط یک شریان کاروتید داخلی با شبکه سمپاتیک در اطراف آن و عصب دورکننده که توسط اندوتلیوم پوشیده شده است، عبور میکند. عصب دورکننده نسبت به شریان در قسمت تحتانی-جانبی قرار دارد.
Structures present in the lateral wall of cavernous sinus The lateral wall of cavernous sinus (between its endothelium and meningeal layer of dura mater) contains (Fig. 16.3) oculomotor, trochlear, ophthalmic and maxillary nerves from above downwards.
ساختارهای موجود در دیواره جانبی سینوس غاری دیواره جانبی سینوس غاری (بین اندوتلیوم و لایه مننژی سختشامه) شامل (شکل 16.3) اعصاب چشمی، قرقرهای، چشمی و فکی از بالا به پایین است.
Communications of the cavernous sinus (Fig. 16.4) Each sinus communicates with the:
ارتباطات سینوس کاورنوس (شکل ۱۶.۴) هر سینوس با موارد زیر ارتباط برقرار میکند:
– facial vein through two routes: (a) via superior ophthalmic and angular veins, and (b) via pterygoid venous plexus and deep facial vein,
– ورید صورت از طریق دو مسیر: (الف) از طریق وریدهای چشمی فوقانی و زاویهای، و (ب) از طریق شبکه وریدی پتریگوئید و ورید عمقی صورت،
– superior sagittal sinus, through superficial middle cerebral vein and superior anastomotic vein,
– سینوس ساژیتال فوقانی، از طریق ورید مغزی میانی سطحی و ورید آناستوموز فوقانی،
– pterygoid venous plexus, through emissary veins passing through foramen ovale, foramen spinosum, foramen vesalii and foramen lacerum,
– شبکه وریدی پتریگوئید، از طریق وریدهای خروجی که از سوراخ بیضی، سوراخ خاردار، سوراخ وزالی و سوراخ لاسروم عبور میکنند،
– transverse sinus, through superior petrosal sinus,
– سینوس عرضی، از طریق سینوس پتروزال فوقانی،
– internal jugular vein, through inferior petrosal sinus,
– ورید ژوگولار داخلی، از طریق سینوس پتروزال تحتانی،
– internal vertebral venous plexus, through basilar venous plexus, and
– شبکه وریدی مهرهای داخلی، از طریق شبکه وریدی بازیلار، و
– opposite cavernous sinus, through anterior and posterior intercavernous sinuses.
– سینوس کاورنوس مقابل، از طریق سینوسهای بین کاورنوس قدامی و خلفی.
Tributaries of the cavernous sinus (Fig. 16.4)
شاخههای سینوس غاری (شکل ۱۶.۴)
• Superior ophthalmic vein, which is often joined by inferior ophthalmic vein.
• ورید افتالمیک فوقانی، که اغلب به ورید افتالمیک تحتانی متصل میشود.
• Inferior ophthalmic vein, if it does not end in the superior ophthalmic vein.
• ورید افتالمیک تحتانی، اگر به ورید افتالمیک فوقانی ختم نشود.
• Sometimes central vein of retina, when it fails to drain into the superior ophthalmic vein.
• گاهی اوقات ورید مرکزی شبکیه، زمانی که نتواند به ورید افتالمیک فوقانی تخلیه شود.
• Superficial middle cerebral vein.
• ورید مغزی میانی سطحی.
• A few inferior cerebral veins.
• تعداد کمی ورید مغزی تحتانی.
• Sphenoparietal sinus.
• سینوس اسفنوپاریتال.
• Sometimes anterior frontal trunk of middle meningeal vein, if it does not drain into the pterygoid venous plexus through foramen ovale, or into the sphenoparietal sinus.
• گاهی اوقات تنه قدامی پیشانی ورید مننژیال میانی، اگر از طریق سوراخ بیضی به شبکه وریدی پتریگوئید یا به سینوس اسفنوپاریتال تخلیه نشود.
Clinical Correlation
• Cavernous sinus thrombosis
The infection reaching the cavernous sinus via emissary veins from face, scalp and paranasal sinuses, etc. may cause cavernous sinus thrombosis which presents with pain in the eye and total ophthalmoplegia due to involvement of IIIrd, IVth and VIth cranial nerves resent inside and in the lateral wall of the cavernous sinus. There may be marked oedema of eyelids due to congestion of orbital veins.
همبستگی بالینی
• ترومبوز سینوس کاورنوس
عفونتی که از طریق وریدهای خروجی از صورت، پوست سر و سینوسهای پارانازال و غیره به سینوس کاورنوس میرسد، ممکن است باعث ترومبوز سینوس کاورنوس شود که با درد چشم و فلج کامل چشم به دلیل درگیری اعصاب جمجمهای سوم، چهارم و ششم که در داخل و دیواره جانبی سینوس کاورنوس قرار دارند، بروز میکند. ممکن است به دلیل احتقان وریدهای حدقه، ادم قابل توجه پلکها وجود داشته باشد.
• Pulsating exophthalmos
In fracture of the base of the skull, the internal carotid artery may rupture within the cavernous sinus, producing an arteriovenous fistula. Consequently, the arterial blood rushes into the cavernous sinus, enlarging it and forcing its blood into communicating veins. As a result, the eyeball protrudes (exophthalmos) and conjunctiva becomes engorged (chemosis) on the side of injury. Interestingly in these circumstances the bulging eye pulsates in synchrony with the radial pulse, producing a clinical condition called pulsating exophthalmos.
• اگزوفتالمی ضرباندار
در شکستگی قاعده جمجمه، شریان کاروتید داخلی ممکن است در سینوس غاری پاره شود و یک فیستول شریانی-وریدی ایجاد کند. در نتیجه، خون شریانی به سینوس غاری هجوم میبرد، آن را بزرگ میکند و خون آن را به رگهای ارتباطی میراند. در نتیجه، کره چشم بیرون میزند (اگزوفتالمی) و ملتحمه در سمت آسیب دیده متورم میشود (کموزیس). جالب اینجاست که در این شرایط، چشم بیرون زده همزمان با نبض رادیال ضربان میزند و یک وضعیت بالینی به نام اگزوفتالمی ضرباندار ایجاد میکند.
Superior petrosal sinus
Superior petrosal sinus lies in the attached border of tentorium cerebelli runs along the superior border of petrous temporal bone and connects the cavernous sinus with the transverse sinus. It drains the cavernous sinus into the transverse sinus.
سینوس پتروزال فوقانی
سینوس پتروزال فوقانی در لبه متصل چادرینه مخچه قرار دارد و در امتداد لبه فوقانی استخوان گیجگاهی پتروس امتداد دارد و سینوس غاری را به سینوس عرضی متصل میکند. این سینوس غاری را به سینوس عرضی تخلیه میکند.
Inferior petrosal sinus
Inferior petrosal sinus lies in the groove between the petrous temporal bone and clivus of sphenoid and drains the cavernous sinus into the bulb of the internal jugular vein.
سینوس پتروزال تحتانی
سینوس پتروزال تحتانی در شیار بین استخوان گیجگاهی پتروس و کلیوس استخوان اسفنوئید قرار دارد و سینوس کاورنوس را به داخل بولب ورید ژوگولار داخلی تخلیه میکند.
Transverse sinuses
Transverse sinuses lie in the posterior attached margins of the tentorium cerebelli, groove the occipital bone. The right transverse sinus is usually a continuation of the superior sagittal sinus while the left one is usually a continuation of straight sinus. Both these sinuses become sigmoid sinuses on the inner aspects of mastoid processes of temporal bones.
سینوسهای عرضی
سینوسهای عرضی در حاشیههای خلفی متصل به چادرینه مخچه قرار دارند و استخوان پسسری را شیار میدهند. سینوس عرضی راست معمولاً ادامه سینوس ساژیتال فوقانی است در حالی که سینوس عرضی چپ معمولاً ادامه سینوس مستقیم است. هر دوی این سینوسها در قسمت داخلی زائدههای ماستوئید استخوانهای گیجگاهی به سینوسهای سیگموئید تبدیل میشوند.
Sigmoid sinuses
Sigmoid sinuses each sigmoid sinus is a continuation of the transverse sinus beyond a point where it leaves the tentorium cerebelli. It lies between the two layers of dura mater of posterior cranial fossa and takes a S-shaped curve posterior to the base of petrous temporal bone producing a S-shaped groove on the mastoid part of temporal bone and jugular process of occipital bone. It passes out through the jugular foramen to continue as internal jugular vein.
سینوسهای سیگموئید
سینوسهای سیگموئید هر سینوس سیگموئید ادامه سینوس عرضی پس از نقطهای است که از چادرینه مخچه خارج میشود. این سینوس بین دو لایه سختشامه حفره جمجمهای خلفی قرار دارد و یک منحنی S شکل در خلف قاعده استخوان گیجگاهی پتروس ایجاد میکند و یک شیار S شکل روی قسمت ماستوئید استخوان گیجگاهی و زائده ژوگولار استخوان پسسری ایجاد میکند. این سینوس از طریق سوراخ ژوگولار خارج میشود تا به عنوان ورید ژوگولار داخلی ادامه یابد.
Clinical Correlation
As the sigmoid sinus is closely related to the mastoid antrum and being separated from it only by a thin plate of bone. The infection from middle ear or mastoid antrum can spread through this thin portion (which may be membranous especially in children) to sigmoid sinus and cause its thrombosis.
همبستگی بالینی
از آنجایی که سینوس سیگموئید ارتباط نزدیکی با آنتروم ماستوئید دارد و فقط توسط یک صفحه نازک استخوانی از آن جدا میشود، عفونت گوش میانی یا آنتروم ماستوئید میتواند از طریق این قسمت نازک (که ممکن است به خصوص در کودکان غشایی باشد) به سینوس سیگموئید گسترش یابد و باعث ترومبوز آن شود.
Arachnoid mater
Arachnoid mater is a thin, transparent membrane lying between the pia mater internally and dura mater externally. It invests the brain loosely and continues as spinal arachnoid at the foramen magnum, which ends at the level of second sacral vertebra. It is closely related to the dura mater. Being closely related to the dura, it bridges over all the fissures on the surface of the brain except two:
ماده عنکبوتیه
ماده عنکبوتیه غشایی نازک و شفاف است که بین نرمشامه در داخل و سختشامه در خارج قرار دارد. این ماده به صورت آزاد مغز را در بر میگیرد و به عنوان آراکنوئید نخاعی در سوراخ بزرگ مغز که در سطح مهره دوم خاجی پایان مییابد، ادامه مییابد. این ماده ارتباط نزدیکی با سختشامه دارد. از آنجایی که ارتباط نزدیکی با سختشامه دارد، روی تمام شیارهای سطح مغز به جز دو شیار پل میزند:
1. Longitudinal cerebral fissure, into which it is carried by the falx cerebri.
2. Stem of lateral sulcus, into which it is pushed by the lesser wing of the sphenoid.
۱. شیار طولی مغز، که توسط داس مغزی به آن منتقل میشود.
۲. ساقه شیار جانبی، که توسط بال کوچک استخوان اسفنوئید به آن رانده میشود.
A capillary interval, the subdural space between the meningeal layer of dura and arachnoid mater is traversed by cerebral veins in their route to the dural venous sinuses.
فضای مویرگی، فضای زیر سختشامه، بین لایه مننژی سختشامه و عنکبوتیه است که توسط وریدهای مغزی در مسیر خود به سینوسهای وریدی سختشامه طی میشود.
Processes of arachnoid
• Arachnoid villi are fine finger-like processes which arise from the surface of arachnoid. They push the dura before them and eventually perforate it to project into the venous sinuses. They are covered by specialised mesothelial cells which convey the CSF to blood stream, thus leading to the absorption of CSF. The arachnoid villi are most numerous along the superior sagittal sinus.
زوائد عنکبوتیه
• پرزهای عنکبوتیه، زوائد ظریف انگشت مانندی هستند که از سطح عنکبوتیه منشأ میگیرند. آنها دورا را به جلو هل میدهند و در نهایت آن را سوراخ میکنند تا به سینوسهای وریدی برسند. آنها توسط سلولهای مزوتلیال تخصصی پوشیده شدهاند که CSF را به جریان خون منتقل میکنند و در نتیجه منجر به جذب CSF میشوند. پرزهای عنکبوتیه بیشتر در امتداد سینوس ساژیتال فوقانی قرار دارند.
• Arachnoid granulations (Pacchionian bodies): With advancing age the arachnoid villi enlarge in size and form pedunculated tufts called arachnoid granulations. Some consider that these are aggregations of arachnoid villi, clumped together, i.e. arachnoid granulations are the large clusters of arachnoid villi. Arachnoid granulations like arachnoid villi are concerned with the absorption of CSF. They project into the venous lacunae of the superior sagittal sinus (Fig. 16.5).
• گرانولاسیونهای عنکبوتیه (اجسام پاچینی): با افزایش سن، پرزهای عنکبوتیه از نظر اندازه بزرگ میشوند و دستههای پایهداری به نام گرانولاسیونهای عنکبوتیه تشکیل میدهند. برخی معتقدند که اینها تجمع پرزهای عنکبوتیه هستند که به هم چسبیدهاند، یعنی گرانولاسیونهای عنکبوتیه، خوشههای بزرگی از پرزهای عنکبوتیه هستند. گرانولاسیونهای عنکبوتیه مانند پرزهای عنکبوتیه در جذب CSF نقش دارند. آنها به داخل لاکوناهای وریدی سینوس ساژیتال فوقانی بیرون زدهاند (شکل 16.5).
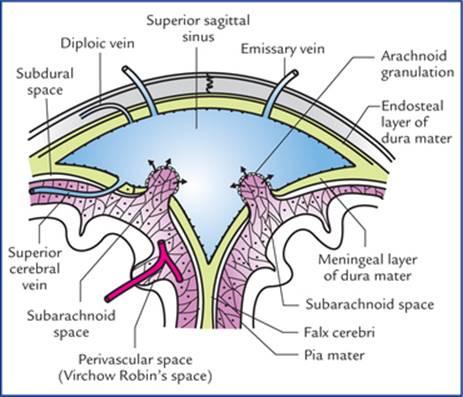
FIG. 16.5 Schematic transverse section through superior sagittal sinus showing arachnoid granulations and absorption of CSF.
شکل ۱۶.۵ برش عرضی شماتیک از سینوس ساژیتال فوقانی که گرانولهای آراکنوئید و جذب CSF را نشان میدهد.
As these granulations enlarge with the age, they produce parasagittal depressions on the inner surface of the cranial vault.
با افزایش سن، این گرانولها فرورفتگیهای پاراساژیتال در سطح داخلی طاق جمجمه ایجاد میکنند.
Clinical Correlation
The meningiomas are tumours arising from arachnoid villi and most commonly occur along the superior sagittal sinus.
همبستگی بالینی
مننژیومها تومورهایی هستند که از پرزهای عنکبوتیه منشأ میگیرند و بیشتر در امتداد سینوس ساژیتال فوقانی رخ میدهند.
Pia mater
Pia mater is thin transparent vascular membrane which closely invests the surface of the brain, i.e. it faithfully follows the surface irregularities of the cerebral hemisphere, and dips in every sulcus forming folds. However, its relationship is not so intimate over the surface of cerebellum where it dips and forms folds only in larger cerebellar fissures.
نرمشامه
نرمشامه یک غشای عروقی نازک و شفاف است که سطح مغز را به طور دقیق پوشش میدهد، یعنی کاملاً از بینظمیهای سطحی نیمکره مغزی پیروی میکند و در هر شیار فرو میرود و چینهایی را تشکیل میدهد. با این حال، ارتباط آن با سطح مخچه چندان نزدیک نیست، جایی که فقط در شیارهای بزرگتر مخچه فرو میرود و چینهایی را تشکیل میدهد.
All the blood vessels to brain run on it before entering the brain.
تمام رگهای خونی مغز قبل از ورود به مغز از روی آن عبور میکنند.
Processes of pia
• Perivascular sheaths around the vessels entering or leaving the brain substance. The large blood vessels of the brain lie in the subarachnoid space. The smaller branches before entering into the substance of brain carry with them the double sleeve of leptomeninges (pia and arachnoid). The outer wall of double sleeve is derived from pia and the inner from the arachnoid (Fig. 16.5). The space between the two layers is called perivascular space (Virchow-Robin’s space).
زوائد نرمشامه
• غلافهای دور عروقی اطراف رگهایی که به ماده مغزی وارد یا از آن خارج میشوند. رگهای خونی بزرگ مغز در فضای زیر عنکبوتیه قرار دارند. شاخههای کوچکتر قبل از ورود به ماده مغزی، غلاف دوگانه لپتومننژ (نرمشامه و عنکبوتیه) را با خود حمل میکنند. دیواره خارجی غلاف دوگانه از نرمشامه و دیواره داخلی از عنکبوتیه مشتق شده است (شکل 16.5). فضای بین این دو لایه، فضای دور عروقی (فضای ویرچو-رابین) نامیده میشود.
• Septa/folds dipping into sulci and fissures of the brain.
• سپتا/چینهایی که به داخل شیارها و شکافهای مغز فرو میروند.
• Tela choroidea of third and fourth ventricles. These are the folds of vascular pia along with ventricular lining the ependyma carried into the interior of the IIIrd and IVth ventricles by developing tuft of blood capillaries. The tela choroidea and tuft of blood capillaries together form choroid plexuses of these ventricles.
• تلا مشیمیه بطنهای سوم و چهارم. اینها چینهای نرمشامه عروقی به همراه پوشش بطنی اپاندیم هستند که با ایجاد دستهای از مویرگهای خونی به داخل بطنهای سوم و چهارم منتقل میشوند.تللا مشیمیه و دستهای از مویرگهای خونی با هم شبکههای مشیمیه این بطنها را تشکیل میدهند.
• Sheaths for cranial nerves.
• غلافهایی برای اعصاب جمجمهای.
Subarachnoid space
Subarachnoid space is the space between the arachnoid mater and pia mater. It is filled with cerebrospinal fluid (CSF) which enters it from ventricular system of the brain.
فضای زیر عنکبوتیه
فضای زیر عنکبوتیه، فضایی بین عنکبوتیه و نرم شامه است. این فضا پر از مایع مغزی نخاعی (CSF) است که از سیستم بطنی مغز وارد آن میشود.
Subarachnoid space is traversed by trabeculae passing from arachnoid to pia, giving it a spider’s web appearance hence the name arachnoid (arachnoid = like spider’s web) and forms a kind of fluid-filled sponge. The arteries and veins of the brain lie in this space.
فضای زیر عنکبوتیه توسط ترابکولهایی که از عنکبوتیه به نرم شامه عبور میکنند، طی میشود و ظاهری شبیه تار عنکبوت به آن میدهد، از این رو نام عنکبوتیه (آراکنوئید = مانند تار عنکبوت) به آن داده است و نوعی اسفنج پر از مایع را تشکیل میدهد. شریانها و وریدهای مغز در این فضا قرار دارند.
Subarachnoid space around the brain is continuous with the subarachnoid space around the spinal cord at foramen magnum, and communicates with the ventricular system only through the foramina in the roof of fourth ventricle.
فضای زیر عنکبوتیه در اطراف مغز با فضای زیر عنکبوتیه در اطراف نخاع در سوراخ بزرگ (foramen magnum) پیوسته است و فقط از طریق سوراخهای سقف بطن چهارم با سیستم بطنی ارتباط برقرار میکند.
Extensions of the subarachnoid space
• A sleeve of the subarachnoid space extends around the optic nerve to the back of the eyeball. Small extensions of the subarachnoid space also occur around the other cranial nerves.
• The subarachnoid space also extends around the arteries and veins of the CNS at points where they penetrate the nervous tissue.
امتدادهای فضای زیر عنکبوتیه
• یک غلاف از فضای زیر عنکبوتیه در اطراف عصب بینایی تا پشت کره چشم امتداد دارد. امتدادهای کوچکی از فضای زیر عنکبوتیه نیز در اطراف سایر اعصاب جمجمهای وجود دارد.
• فضای زیر عنکبوتیه همچنین در اطراف شریانها و وریدهای سیستم عصبی مرکزی در نقاطی که به بافت عصبی نفوذ میکنند، امتداد مییابد.
Subarachnoid cisterns (Fig. 16.6)
The arachnoid mater bridges over the sulci on the surfaces of the brain. In certain situations, for example, at the base of the brain, around the brainstem and cerebellum, around the free margin of tentorium cerebelli, and in association with major blood vessels, the arachnoid and pia are widely separated. Thus subarachnoid space presents dilatations, filled with substantial amount of CSF called subarachnoid cisterns. These cisterns are large pools of CSF and act as a water-bed to the brain. The important cisterns are discussed as under:
مخازن زیر عنکبوتیه (شکل 16.6)
ماده عنکبوتیه روی شیارهای روی سطوح مغز پل میزند. در موقعیتهای خاص، به عنوان مثال، در پایه مغز، اطراف ساقه مغز و مخچه، اطراف حاشیه آزاد چادرینه مخچه، و در ارتباط با رگهای خونی اصلی، عنکبوتیه و نرمشامه به طور گسترده از هم جدا میشوند. بنابراین فضای زیر عنکبوتیه دارای اتساع است که با مقدار قابل توجهی مایع مغزی نخاعی پر شده و مخازن زیر عنکبوتیه نامیده میشوند. این مخازن، مخازن بزرگی از مایع مغزی نخاعی هستند و به عنوان یک بستر آبی برای مغز عمل میکنند. مخازن مهم در زیر مورد بحث قرار گرفتهاند:
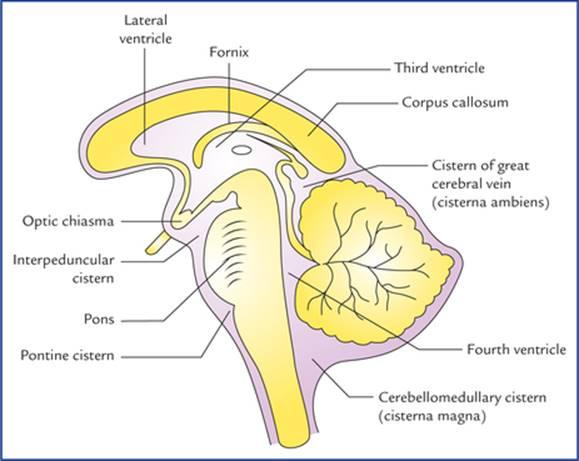
FIG. 16.6 Sagittal section of brain showing location of principal subarachnoid cisterns.
شکل ۱۶.۶ برش ساژیتال مغز که محل مخازن اصلی زیر عنکبوتیه را نشان میدهد.
• Cerebellomedullary cistern (cisterna magna). It is the largest cistern and formed by the arachnoid, bridging the interval between the medulla oblongata and the inferior surface of the cerebellum. Thus it lies in the angle formed by the cerebellum, the medulla oblongata and the occipital bone.
• مخزن مخچه-مدولا (سیسترنا ماگنا). این بزرگترین مخزن است و توسط عنکبوتیه تشکیل شده و فاصله بین بصل النخاع و سطح تحتانی مخچه را پر میکند. بنابراین در زاویهای که توسط مخچه، بصل النخاع و استخوان پسسری تشکیل میشود، قرار دارد.
It is directly continuous inferiorly with the posterior part of the spinal subarachnoid space.
این مخزن مستقیماً از پایین با قسمت خلفی فضای زیر عنکبوتیه نخاعی امتداد دارد.
Clinical Correlation
The cerebellomedullary cistern is easily accessible to a needle introduced anterosuperiorly through the posterior atlanto-occipital membrane, between the posterior arch of atlas and posterior margin of the foramen magnum. Therefore, it is utilized; for cisternal puncture if lumbar puncture is not possible to withdraw CSF by clinicians for therapeutic and diagnostic purposes.
همبستگی بالینی
سیسترن مخچه-بصل النخاع به راحتی برای سوزنی که از طریق غشای خلفی آتلانتو-اکسیپیتال، بین قوس خلفی اطلس و لبه خلفی سوراخ بزرگ، به صورت قدامی-فوقانی وارد میشود، قابل دسترسی است. بنابراین، در صورتی که امکان برداشت CSF توسط پزشکان برای اهداف درمانی و تشخیصی با سوراخ کردن کمری وجود نداشته باشد، برای سوراخ کردن سیسترن استفاده میشود.
This cistern is triangular in sagittal section. It is the only cistern which directly communicates with the ventricular system of the brain through openings (foramen of Magendie and foramina of Luschka) in the roof of the fourth ventricle.
این سیسترن در مقطع ساژیتال مثلثی شکل است. این تنها سیسترنی است که مستقیماً از طریق روزنههایی (سوراخ ماژندی و سوراخ لوشکا) در سقف بطن چهارم با سیستم بطنی مغز ارتباط برقرار میکند.
• Pontine cistern (cisterna pontis): This is an extensive subarachnoid space on the ventral surface of the pons and contains the basilar artery and its branches. It is continuous below with the subarachnoid space of the spinal cord, behind with the cerebellomedullary cistern and rostrally with the interpeduncular cistern.
• سیسترن پونتین (cisterna pontis): این یک فضای زیر عنکبوتیه گسترده در سطح شکمی پل مغزی است و شامل شریان بازیلار و شاخههای آن میشود. این فضا در پایین با فضای زیر عنکبوتیه نخاع، در پشت با سیسترن مخچه-مغزی و در جلو با سیسترن بین پایهای (interpeduncular) پیوسته است.
• Interpeduncular cistern (basal cistern): It is formed by the arachnoid bridging across the two temporal lobes and contains the circle of Willis (circulus arteriosus).
• سیسترن بین پایهای (سیسترن قاعدهای): از اتصال عنکبوتیه بین دو لوب گیجگاهی تشکیل شده و شامل حلقه ویلیس (سیرکولوس آرتریوزوس) است.
Interpeduncular cistern is continuous laterally with the subarachnoid spaces surrounding the middle and posterior cerebral arteries, and anteriorly with the subarachnoid spaces around the anterior cerebral arteries.
سیسترن بین پایهای از طرفین با فضاهای زیر عنکبوتیه اطراف شریانهای مغزی میانی و خلفی و از جلو با فضاهای زیر عنکبوتیه اطراف شریانهای مغزی قدامی پیوسته است.
• Cistern of lateral sulcus/fossa (sylvian cistern): It lies in front of each temporal pole and is formed by arachnoid bridging the lateral sulcus. It contains the middle cerebral artery.
• سیسترن شیار/حفره جانبی (سیسترن سیلویان): در جلوی هر قطب گیجگاهی قرار دارد و از پل زدن عنکبوتیه روی شیار جانبی تشکیل شده است. این سیسترن حاوی شریان مغزی میانی است.
• Cistern of great cerebral vein (cisterna superior or cisterna ambiens): It occupies the interval between the splenium of corpus callosum and the superior surface of cerebellum. This cistern contains the great cerebral vein of Galen and pineal gland, and is widely used as a neurosurgical landmark.
• سیسترن ورید مغزی بزرگ (سیسترن فوقانی یا سیسترن آمبیانس): فاصله بین طحال جسم پینهای و سطح فوقانی مخچه را اشغال میکند. این سیسترن حاوی ورید مغزی بزرگ گالن و غده پینه آل است و به عنوان یک نقطه عطف جراحی مغز و اعصاب به طور گسترده مورد استفاده قرار میگیرد.
The various cisterns are large pools of CSF and communicate freely with each other. The pulsations of arteries within CSF help to force the CSF from cisterns on to the superolateral surfaces of the cerebral hemispheres and then into arachnoid villi and granulations.
سیسترنهای مختلف، مخازن بزرگی از مایع مغزی نخاعی (CSF) هستند و آزادانه با یکدیگر ارتباط دارند. ضربانهای شریانهای درون CSF به راندن CSF از سیسترنها به سطوح فوقانی-جانبی نیمکرههای مغزی و سپس به پرزها و گرانولهای عنکبوتیه کمک میکند.
The summary of various cisterns is given in Table 16.3.
خلاصه سیسترنهای مختلف در جدول 16.3 آمده است.
Table 16.3
Location and vascular contents of various cisterns of the brain
جدول 16.3
محل و محتوای عروقی سیسترنهای مختلف مغز
Cistern | Location | Contents |
Cerebellomedullary cistern/cisterna magna | In the interval between medulla oblongata and inferior surface of cerebellum | – |
Pontine cistern/cisterna pontis | On the ventral surface of pons | Basilar artery and its branches |
Interpeduncular cistern/basal cistern | At the base of brain in the interval between two temporal lobes | Circle of Willis (circulus arteriosus) |
Cistern of lateral sulcus/sylvian cistern | In the stem of lateral sulcus in front of temporal pole | Middle cerebral artery |
Cistern of great cerebral vein of Galen/ cisterna ambiens | In the interval between splenium of corpus callosum and superior surface of cerebellum | Great cerebral vein of Galen |
Cerebrospinal Fluid
Cerebrospinal fluid (CSF) is somewhat similar to that of blood plasma and interstitial fluid. It is present in the ventricular system within the CNS and in the subarachnoid space surrounding the CNS. It bathes both the external and internal surfaces of the brain and spinal cord and provides a protective cushion between the CNS and the surrounding bones.
مایع مغزی نخاعی
مایع مغزی نخاعی (CSF) تا حدودی شبیه به پلاسمای خون و مایع میانبافتی است. این مایع در سیستم بطنی درون سیستم عصبی مرکزی (CNS) و در فضای زیر عنکبوتیه اطراف سیستم عصبی مرکزی (CNS) وجود دارد. این مایع سطوح خارجی و داخلی مغز و نخاع را میپوشاند و یک لایه محافظ بین سیستم عصبی مرکزی و استخوانهای اطراف آن ایجاد میکند.
In an adult, the total volume of CSF is about 150 ml, out of which only 30 ml is in the ventricular system and remainder in the subarachnoid space.
در یک بزرگسال، حجم کل CSF حدود ۱۵۰ میلیلیتر است که از این مقدار تنها ۳۰ میلیلیتر در سیستم بطنی و بقیه در فضای زیر عنکبوتیه قرار دارد.
Composition
Cerebrospinal fluid is clear, colourless and slightly alkaline fluid with a specific gravity of 1005-1008. It contains inorganic salts, and traces of protein and glucose similar to that of blood plasma. But, it has much lower protein content than the plasma and the glucose content is about half to that of blood, the chloride content is slightly more in CSF (Table 16.4).
ترکیب
مایع مغزی نخاعی مایعی شفاف، بیرنگ و کمی قلیایی با وزن مخصوص 1005-1008 است. این مایع حاوی نمکهای معدنی و مقادیر کمی پروتئین و گلوکز مشابه پلاسمای خون است. اما محتوای پروتئین آن بسیار کمتر از پلاسما و محتوای گلوکز آن تقریباً نصف خون است، محتوای کلرید در CSF کمی بیشتر است (جدول 16.4).
Table 16.4
Composition of CSF and blood plasma
جدول 16.4
ترکیب CSF و پلاسمای خون
Substance | CSF | Plasma |
Protein | 25 mg/100 ml | 600 mg/100 ml |
Glucose | 50 mg/100 ml | 100 mg/100 ml |
Chloride | 120 mEq/L | 100 mEq/L |
CSF = cerebrospinal fluid
CSF = مایع مغزی نخاعی
Clinical Correlation
Normally the CSF is clear and colourless with specific gravity of 1005–1008, and is almost cell-free having only 0–5 lymphocytes/mm3. In bacterial meningitis, the fluid is cloudy, with raised protein content and vastly increased number of cells.
همبستگی بالینی
به طور معمول، مایع مغزی نخاعی (CSF) شفاف و بیرنگ با وزن مخصوص 1005-1008 است و تقریباً بدون سلول بوده و تنها 0-5 لنفوسیت در میلیمتر مکعب دارد 3. در مننژیت باکتریایی، مایع کدر است و محتوای پروتئین آن افزایش یافته و تعداد سلولها به طور قابل توجهی افزایش یافته است.
Analysis of CSF has diagnostic value in many diseases of CNS.
آنالیز CSF در بسیاری از بیماریهای سیستم عصبی مرکزی (CNS) ارزش تشخیصی دارد.
Production
About 80 to 90% of the CSF is produced by the choroid plexuses within the lateral ventricles, with remaining being produced by the choroid plexuses in the third and fourth ventricles. The process of production whether by secretion, filtration, or dialyzation is uncertain. The average amount of CSF formed per day is about 500 ml.
تولید
حدود ۸۰ تا ۹۰ درصد مایع مغزی نخاعی (CSF) توسط شبکههای مشیمیه در بطنهای جانبی تولید میشود و بقیه توسط شبکههای مشیمیه در بطنهای سوم و چهارم تولید میشود. فرآیند تولید، چه از طریق ترشح، فیلتراسیون یا دیالیز، نامشخص است. میانگین مقدار CSF تولید شده در روز حدود ۵۰۰ میلیلیتر است.
Circulation and Absorption (Fig. 16.7)
The CSF is produced mainly in the lateral ventricles, from where it passes through the interventricular foramina (of Monro) into the third ventricle, and then via cerebral aqueduct into the fourth ventricle. Here the fluid escapes via the median aperture (foramen of Magendie) and lateral apertures (foramina of Luschka) in the roof of lateral ventricle, into the cerebellomedullary and pontine cisterns respectively. From these sites the fluid flows slowly in the subarachnoid space over the brain and spinal cord.
گردش خون و جذب (شکل ۱۶.۷)
مایع مغزی نخاعی عمدتاً در بطنهای جانبی تولید میشود، از آنجا از طریق سوراخهای بین بطنی (مونرو) به بطن سوم و سپس از طریق مجرای مغزی به بطن چهارم میرود. در اینجا مایع از طریق روزنه میانی (سوراخ ماژندی) و روزنههای جانبی (سوراخ لوشکا) در سقف بطن جانبی، به ترتیب به مخازن مخچهای-مغزی و پل مغزی میریزد. از این محلها، مایع به آرامی در فضای زیر عنکبوتیه روی مغز و نخاع جریان مییابد.
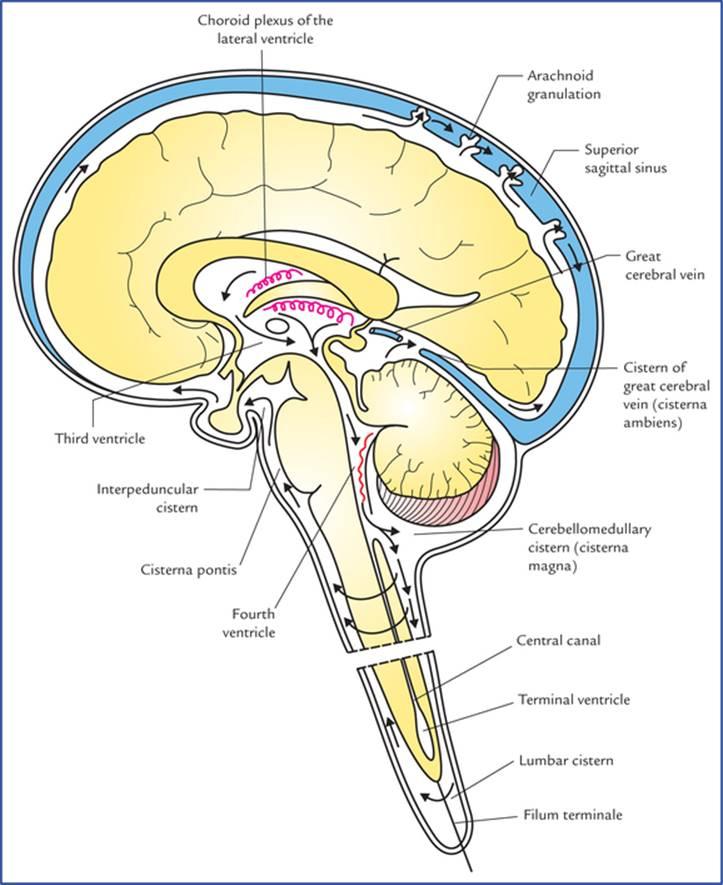
FIG. 16.7 Circulation of cere-brospinal fluid from its sites of formation in the choroid plexuses of lateral ventricle to its sites of absorption into the superior sagittal sinus. Note the location of various cisterns.
شکل ۱۶.۷ گردش مایع مغزی-نخاعی از محل تشکیل آن در شبکههای مشیمیه بطن جانبی تا محل جذب آن در سینوس ساژیتال فوقانی. به محل مخازن مختلف توجه کنید.
Most of the CSF flows upwards through the gap in the tentorium cerebelli and then forwards and laterally over the inferior surface of the cerebrum. Finally, it ascends on the superolateral aspect of each cerebral hemisphere to reach the arachnoid villi and granulations which penetrate into the superior sagittal sinus. The CSF enters into the blood stream of the sinus through the mesothelial cell lining of these villi and granulations.
بیشتر مایع مغزی-نخاعی از طریق شکاف چادرینه مخچه به سمت بالا و سپس به جلو و به سمت خارج روی سطح تحتانی مخ جریان مییابد. در نهایت، از سطح فوقانی-جانبی هر نیمکره مغزی بالا میرود تا به پرزها و گرانولهای عنکبوتیه برسد که به سینوس ساژیتال فوقانی نفوذ میکنند. مایع مغزی-نخاعی از طریق پوشش سلولی مزوتلیال این پرزها و گرانولها وارد جریان خون سینوس میشود.
Some of the CSF moves inferiorly in the subarachnoid space around the spinal cord and cauda equina.
مقداری از مایع مغزی-نخاعی در فضای زیر عنکبوتیه اطراف نخاع و دم اسب به سمت پایین حرکت میکند.
Small amount of absorption may also occur into the pial veins.
مقدار کمی از جذب نیز ممکن است در وریدهای پیال رخ دهد.
The flow of CSF is facilitated by the pulsations of cerebral and spinal arteries present in the subarachnoid space, and the movements of the head and spine.
جریان CSF توسط ضربانهای شریانهای مغزی و نخاعی موجود در فضای زیر عنکبوتیه و حرکات سر و ستون فقرات تسهیل میشود.
The circulation and absorption of CSF is summarized in Flowchart 16.1.
گردش و جذب CSF در نمودار جریان ۱۶.۱ خلاصه شده است.
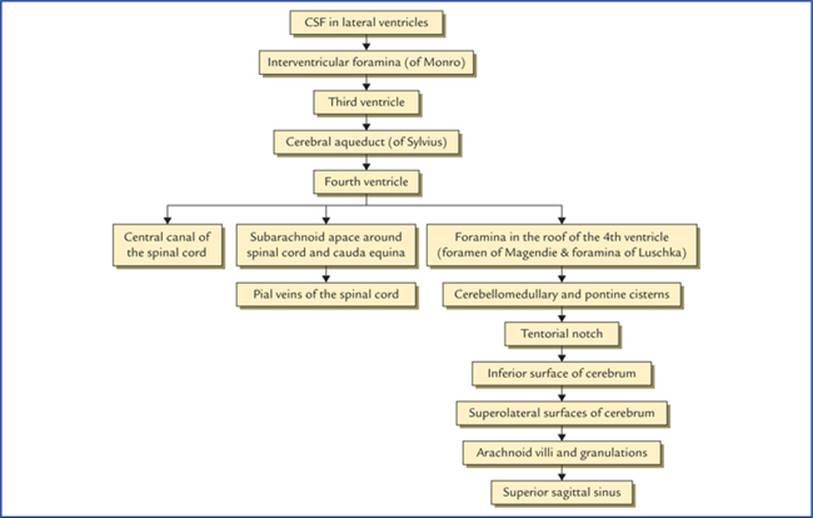
FLOWCHART 16.1 Circulation and absorption of CSF.
نمودار جریان ۱۶.۱ گردش و جذب CSF.
Functions of CSF
وظایف مایع مغزی نخاعی
• It serves as a cushion between the CNS and surrounding bones.
• به عنوان یک ضربه گیر بین سیستم عصبی مرکزی (CNS) و استخوانهای اطراف عمل میکند.
• CSF acts as a shock absorber (i.e. it prevents or diminishes the transmission of jarring or shocking forces to the CNS).
• مایع مغزی نخاعی (CSF) به عنوان یک ضربه گیر عمل میکند (یعنی از انتقال نیروهای ضربهای یا تکان دهنده به سیستم عصبی مرکزی جلوگیری میکند یا آن را کاهش میدهد).
• It supports the brain and spinal cord, and maintains a uniform pressure upon them. The brain simply floats in the CSF, and it has been stated that a brain weighing 1,500g in air, weighs no more than 50g in cerebrospinal fluid.
• از مغز و نخاع پشتیبانی میکند و فشار یکنواختی را بر آنها حفظ میکند. مغز به سادگی در مایع مغزی نخاعی شناور است و گفته شده است که وزن مغز در هوا ۱۵۰۰ گرم است و وزن آن در مایع مغزی نخاعی بیش از ۵۰ گرم نیست.
• Change in the intracranial volume is sometimes compensated by the controlled production and absorption of CSF. For example, if blood volume of the brain increases then more CSF drains away. Conversely if brain’s blood volume reduces, more CSF is retained.
• تغییر در حجم داخل جمجمه گاهی اوقات با تولید و جذب کنترل شده مایع مغزی نخاعی جبران میشود. به عنوان مثال، اگر حجم خون مغز افزایش یابد، مایع مغزی نخاعی بیشتری تخلیه میشود. برعکس، اگر حجم خون مغز کاهش یابد، مایع مغزی نخاعی بیشتری حفظ میشود.
• It nourishes the CNS.
• سیستم عصبی مرکزی (CNS) را تغذیه میکند.
• CSF removes the metabolites (waste products) from the CNS.
• مایع مغزی نخاعی (CSF) متابولیتها (مواد زائد) را از سیستم عصبی مرکزی (CNS) خارج میکند.
• It serves as a pathway for pineal secretions to reach the pituitary gland.
• به عنوان مسیری برای رسیدن ترشحات غده صنوبری به غده هیپوفیز عمل میکند.
Special Properties of CSF
1. Due to presence of blood-CSF barrier:
• Antibodies are not found in the CSF hence infections of the CNS are often fatal.
• Bile is not found in CSF, even in severe jaundice.
• Most of the drugs cannot reach CSF.
خواص ویژه مایع مغزی نخاعی (CSF)
1. به دلیل وجود سد خونی-مایع مغزی نخاعی:
• آنتیبادیها در مایع مغزی نخاعی یافت نمیشوند، بنابراین عفونتهای سیستم عصبی مرکزی اغلب کشنده هستند.
• صفرا حتی در زردی شدید در مایع مغزی نخاعی یافت نمیشود.
• اکثر داروها نمیتوانند به مایع مغزی نخاعی برسند.
2. There is no CSF-brain barrier, hence if drugs are injected into the subarachnoid space (intrathecal injections) they soon enter the extracellular spaces around the neurons and neuroglia.
۲. هیچ سدی بین مایع مغزی نخاعی و مغز وجود ندارد، بنابراین اگر داروها به فضای زیر عنکبوتیه (تزریق داخل نخاعی) تزریق شوند، به زودی وارد فضاهای خارج سلولی اطراف نورونها و نوروگلیا میشوند.
N.B. It has been shown that inflammation increases the diffusion rate of penicillin into the CSF. The opinions of paediatricians are, therefore, divided as to whether intrathecal therapy is necessary in the treatment of pyogenic conditions affecting the meninges.
توجه: نشان داده شده است که التهاب، میزان انتشار پنیسیلین به مایع مغزی نخاعی را افزایش میدهد. بنابراین، نظرات متخصصان اطفال در مورد اینکه آیا درمان داخل نخاعی در درمان بیماریهای چرکی مؤثر بر مننژ ضروری است یا خیر، متفاوت است.
Clinical Correlation
• Cerebrospinal fluid can be obtained by lumbar, cisternal or ventricular puncture. The first method (i.e. lumbar puncture) being the easiest, is commonly used by the clinicians for taking out the CSF for various diagnostic and therapeutic purposes (see Chapter 7).
همبستگی بالینی
• مایع مغزی نخاعی را میتوان از طریق پونکسیون کمری، سیسترنال یا بطنی به دست آورد. روش اول (یعنی پونکسیون کمری) که سادهترین روش است، معمولاً توسط پزشکان برای گرفتن CSF برای اهداف مختلف تشخیصی و درمانی استفاده میشود (به فصل 7 مراجعه کنید).
• Froin’s syndrome (also called loculation syndrome) If a block occurs anywhere in the vertebral canal preventing fluid passing the obstruction, the CSF below the obstruction shows following special properties:
– It coagulates spontaneously as the amount of protein in it is greatly increased.
– It may be yellow in colour like plasma (xantho-chromia) due to altered blood pigment.
– Sudden increase of intracranial venous pressure is not transmitted to the CSF below the level of block.
• سندرم فروین (که سندرم لوکولاسیون نیز نامیده میشود) اگر انسدادی در هر جایی از کانال مهرهای رخ دهد که مانع عبور مایع از محل انسداد شود، مایع مغزی نخاعی زیر محل انسداد ویژگیهای خاص زیر را نشان میدهد:
– به دلیل افزایش شدید مقدار پروتئین موجود در آن، خود به خود منعقد میشود.
– ممکن است به دلیل تغییر رنگدانههای خون، مانند پلاسما زرد رنگ (زانتو کرومیا) باشد.
– افزایش ناگهانی فشار وریدی داخل جمجمه به مایع مغزی نخاعی زیر سطح انسداد منتقل نمیشود.
• Hydrocephalus
Hydrocephalus is an abnormal increase in the volume of cerebrospinal fluid (CSF) within the skull. It is characterized by excessive accumulation of CSF in the cerebral ventricles or subarachnoid space.
• هیدروسفالی
هیدروسفالی افزایش غیرطبیعی حجم مایع مغزی نخاعی (CSF) در داخل جمجمه است. این بیماری با تجمع بیش از حد CSF در بطنهای مغزی یا فضای زیر عنکبوتیه مشخص میشود.
Causes
– Excessive production of CSF.
– Obstruction in some part of the circulatory route of CSF.
– Interference with the absorption of the CSF.
علل
– تولید بیش از حد مایع مغزی نخاعی.
– انسداد در بخشی از مسیر گردش مایع مغزی نخاعی.
– تداخل در جذب مایع مغزی نخاعی.
Out of these three factors, the obstruction in some part of the circulatory route of CSF is the common cause. The obstruction may occur at one of the following two sites:
(a) Inside the ventricular system: The common sites of block are: interventricular foramina of Monro, aqueduct of Sylvius, foramina of Magendie and Luschka in the roof of fourth ventricle.
(b) Obstruction at the interventricular foramina leads to distension of one or both lateral ventricles depending upon whether one or both foramina are blocked.
از بین این سه عامل، انسداد در بخشی از مسیر گردش مایع مغزی نخاعی (CSF) علت شایع است. انسداد ممکن است در یکی از دو محل زیر رخ دهد:
(الف) داخل سیستم بطنی: محلهای شایع انسداد عبارتند از: سوراخهای بین بطنی مونرو، قنات سیلویوس، سوراخهای ماژندی و لوشکا در سقف بطن چهارم.
(ب) انسداد در سوراخهای بین بطنی منجر به اتساع یک یا هر دو بطن جانبی میشود، بسته به اینکه یک یا هر دو سوراخ مسدود شده باشند.
– Obstruction of the aqueduct of Sylvius leads to distension of both lateral ventricles and third ventricle.
– Obstruction at the openings in the roof of fourth ventricle leads to distension of all the ventricles.
– انسداد مجرای سیلویوس منجر به اتساع هر دو بطن جانبی و بطن سوم میشود.
– انسداد در دهانههای سقف بطن چهارم منجر به اتساع تمام بطنها میشود.
At the opening in the tentorium cerebelli: If the sub-arachnoid space surrounding midbrain passing through the tentorial notch is blocked due to adhesions, the CSF from below the tentorium cannot flow upwards through the tentorial notch and spread over the surfaces of the cerebral hemisphere to reach the arachnoid granulations for absorption.
در دهانه چادرینه مخچه: اگر فضای زیر عنکبوتیه اطراف مغز میانی که از بریدگی چادرینه عبور میکند به دلیل چسبندگی مسدود شود، مایع مغزی نخاعی از زیر چادرینه نمیتواند از طریق بریدگی چادرینه به سمت بالا جریان یابد و روی سطوح نیمکره مغزی پخش شود تا برای جذب به گرانولهای عنکبوتیه برسد.
Types of Hydrocephalus
Two varieties of hydrocephalus are described: (a) non-communicating, and (b) communicating.
انواع هیدروسفالی
دو نوع هیدروسفالی شرح داده شده است: (الف) غیر ارتباطی و (ب) ارتباطی.
If the CSF accumulates within the ventricular system the condition is called internal (non-communicating) hydrocephalus. It occurs due to blockage at some point between its site of formation at the choroid plexuses and its site of exit through the foramina in the roof of fourth ventricle.
اگر مایع مغزی نخاعی در داخل سیستم بطنی تجمع یابد، این وضعیت هیدروسفالی داخلی (غیر ارتباطی) نامیده میشود. این وضعیت به دلیل انسداد در نقطهای بین محل تشکیل آن در شبکههای کوروئید و محل خروج آن از طریق سوراخهای سقف بطن چهارم رخ میدهد.
If the CSF accumulates in the subarachnoid space, the condition is called external (communicating) hydrocephalus as there is no obstruction within or to the outflow from the ventricular system. It commonly occurs due to blockage of arachnoid villi and granulations (e.g. adhesions after meningitis).
اگر مایع مغزی نخاعی در فضای زیر عنکبوتیه تجمع یابد، این وضعیت هیدروسفالی خارجی (ارتباطی) نامیده میشود زیرا هیچ مانعی در داخل یا در مسیر خروج از سیستم بطنی وجود ندارد. این وضعیت معمولاً به دلیل انسداد پرزهای عنکبوتیه و گرانولاسیونها (مثلاً چسبندگی پس از مننژیت) رخ میدهد.
N.B. The hydrocephalus is most commonly caused by the stenosis of the cerebral aqueduct.
توجه: هیدروسفالی معمولاً در اثر تنگی مجرای مغزی ایجاد میشود.
Clinical features of hydrocephalus in infants and children (Fig. 16.8)
ویژگیهای بالینی هیدروسفالی در نوزادان و کودکان (شکل ۱۶.۸)
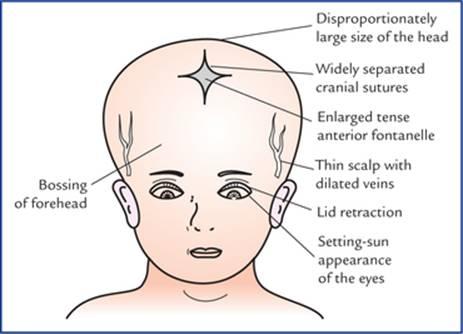
FIG. 16.8 Clinical features of hydrocephalus in infants and young children.
شکل 16.8 ویژگیهای بالینی هیدروسفالی در نوزادان و کودکان خردسال.
1. Disproportionately large size of the head (increased skull circumference).
۱. اندازه نامتناسب سر (افزایش محیط جمجمه).
2. Bossing of the forehead.
۲. برآمدگی پیشانی.
3. Widely separated cranial sutures.
۳. درزهای جمجمه با فاصله زیاد از هم.
4. Enlarged and tense anterior fontanelle.
۴. فونتانل قدامی بزرگ و سفت.
5. Thin scalp with dilated scalp veins.
۵. پوست سر نازک با رگهای گشاد شده پوست سر.
6. Eyes look downwards giving a typical setting-sun appearance.
۶. نگاه چشمها به سمت پایین است که ظاهری شبیه غروب آفتاب ایجاد میکند.
7. Cracked-pot sound on skull percussion.
۷. صدای ترک خوردن گلدان در ضربه به جمجمه.
8. Cranial nerve paralyses are common.
۸. فلج اعصاب جمجمهای شایع است.
9. Progressive loss of motor function.
۹. از دست دادن پیشرونده عملکرد حرکتی.
10. Dementia.
۱۰. زوال عقل.
N.B. There is a natural tendency to the arrest of infantile hydrocephalus. Cuvier and Helmholtz were the cases of arrested hydrocephalus.
توجه: تمایل طبیعی به توقف هیدروسفالی نوزادی وجود دارد. کوویه و هلمهولتز موارد توقف هیدروسفالی بودند.
Clinical Problems
مشکلات بالینی
1. Explain, why the right internal jugular vein is larger than left?
1. توضیح دهید که چرا ورید ژوگولار داخلی راست بزرگتر از ورید ژوگولار داخلی چپ است؟
2. Explain, how the blood-clot or thrombus from pelvic veins after child birth can reach the intracranial dural venous sinuses without passing through the heart and lungs.
2. توضیح دهید که چگونه لخته خون یا ترومبوز از وریدهای لگنی پس از تولد کودک میتواند بدون عبور از قلب و ریهها به سینوسهای وریدی سختشامه داخل جمجمه برسد.
3. Explain, why CNS infections are usually fatal?
3. توضیح دهید که چرا عفونتهای سیستم عصبی مرکزی معمولاً کشنده هستند؟
4. Explain, why removal of CSF by lumbar puncture or cisternal puncture may cause severe headache afterwards?
4. توضیح دهید که چرا برداشتن CSF از طریق سوراخ کردن کمر یا سوراخ کردن سیسترن ممکن است باعث سردرد شدید پس از آن شود؟
5. What is Queckenstedt’s test?
5. آزمایش کوئکنستد چیست؟
6. What are presenting features of a hydrocephalus in infants and children?
6. ویژگیهای بارز هیدروسفالی در نوزادان و کودکان چیست؟
7. What are the usual sites of blockage in the circulatory route of CSF.
7. محلهای معمول انسداد در مسیر گردش خون CSF کدامند.
Clinical Problem Solving
حل مسئله بالینی
1. This is because, the right internal jugular vein is the continuation of larger superior sagittal sinus (superior sagittal sinus → right transverse sinus → right sigmoid sinus → right internal jugular vein) whereas the left internal jugular vein, is the continuation of smaller inferior sagittal sinus (inferior sagittal sinus → left transverse sinus → left sigmoid sinus → left internal jugular vein).
۱. دلیل این امر این است که ورید ژوگولار داخلی راست ادامه سینوس ساژیتال فوقانی بزرگتر است (سینوس ساژیتال فوقانی → سینوس عرضی راست → سینوس سیگموئید راست → ورید ژوگولار داخلی راست) در حالی که ورید ژوگولار داخلی چپ، ادامه سینوس ساژیتال تحتانی کوچکتر است (سینوس ساژیتال تحتانی → سینوس عرضی چپ → سینوس سیگموئید چپ → ورید ژوگولار داخلی چپ).
2. The pelvic veins drain into vertebral venous plexus which communicates with the basilar venous plexus, which in turn communicates with the intracranial dural venous sinuses. All these venous channels are valveless, therefore if intra-abdominal pressure is increased too much (such as during child birth), the clot or thrombus from pelvic veins are directly pushed into the intracranial dural venous sinuses without going through the heart and lung.
۲. وریدهای لگنی به شبکه وریدی مهرهای تخلیه میشوند که با شبکه وریدی بازیلار ارتباط دارد، که به نوبه خود با سینوسهای وریدی سختشامه داخل جمجمهای ارتباط دارد. همه این کانالهای وریدی بدون دریچه هستند، بنابراین اگر فشار داخل شکمی بیش از حد افزایش یابد (مانند هنگام زایمان)، لخته یا ترومبوز از وریدهای لگنی مستقیماً به سینوسهای وریدی سختشامه داخل جمجمهای رانده میشود بدون اینکه از قلب و ریه عبور کند.
3. The CNS infections are usually fatal because there are no antibodies in the CSF. Further, a clinician has a limited choice of antibiotics to give due to presence of blood-brain and blood-CSF barriers.
۳. عفونتهای سیستم عصبی مرکزی معمولاً کشنده هستند زیرا هیچ آنتیبادی در مایع مغزی نخاعی (CSF) وجود ندارد. علاوه بر این، پزشک به دلیل وجود موانع خونی-مغزی و خونی-CSF، انتخاب محدودی از آنتیبیوتیکها برای تجویز دارد.
4. Normally the brain floats freely in CSF but when CSF is removed, the brain sags and hangs on vessels and cranial nerve roots. The traction of these structures stimulate pain fibres producing dragging pain.
۴. مغز به طور معمول آزادانه در مایع مغزی نخاعی شناور است، اما وقتی مایع مغزی نخاعی برداشته میشود، مغز آویزان شده و به رگها و ریشههای عصبی جمجمهای آویزان میشود. کشش این ساختارها، فیبرهای درد را تحریک کرده و باعث درد کششی میشود.
5. When the internal jugular veins are compressed in the neck, there is rise in cerebral venous pressure which inhibits the absorption of CSF into the dural venous sinuses. Consequently there occurs a prompt rise in manometric reading of the CSF pressure. If it does not happen, it indicates blockage in the subarachnoid space (positive Queckenstedt’s test).
۵. هنگامی که وریدهای ژوگولار داخلی در گردن فشرده میشوند، فشار وریدی مغز افزایش مییابد که مانع جذب مایع مغزی نخاعی به سینوسهای وریدی سختشامه میشود. در نتیجه، افزایش سریع فشار CSF در مانومتری رخ میدهد. اگر این اتفاق نیفتد، نشان دهنده انسداد در فضای زیر عنکبوتیه است (آزمایش کوئکنستد مثبت).
6. See page 197.
۶. صفحه ۱۹۷ را ببینید
7. These are: 1. Interventricular foramina, 2. Cerebral aqueduct, 3. Foramina in the roof of fourth ventricle and 4. Subarachnoid space around the midbrain in the tentorial notch.
۷. این موارد عبارتند از: ۱. سوراخهای بین بطنی، ۲. قنات مغزی، ۳. سوراخهای سقف بطن چهارم و ۴. فضای زیر عنکبوتیه در اطراف مغز میانی در بریدگی چادرینه.
Textbook of Clinical Neuroanatomy, 2 ed
Chapter 1. Development of the Nervous System
Chapter 2. Organization and Functions of the Nervous System
Chapter 3. Peripheral Nerves and Ganglia
Chapter 4. Receptors and Effectors
Chapter 5. Dermatomes and Muscular Activity
Chapter 6. Central Nervous System: an Overview
Chapter 7. Spinal Cord
Chapter 8. Brainstem
Chapter 9. Nuclei, Functional Components and Distribution of Cranial Nerves
Chapter 10. Cerebellum and Fourth Ventricle
Chapter 11. Diencephalon and Third Ventricle
Chapter 12. Cerebrum
Chapter 13. Basal Nuclei (Basal Ganglia)
Chapter 14. White Matter of the Cerebrum and Lateral Ventricles
Chapter 15. Blood Supply of the Brain
Chapter 16. Meninges And Cerebrospinal Fluid
Chapter 17. Somatic Motor and Sensory Pathways
Chapter 18. Special Senses and their Neural Pathways
Chapter 19. Reticular Formation and Limbic System
Chapter 20. Autonomic Nervous System
